Orofacial Cleft: What you need to know!

{kind=link}
Good day dear reader of my blog.I hope you are doing great! Today I am going to be discussing a common birth defect condition that we all see around which is orofacial cleft.
What is a Cleft?
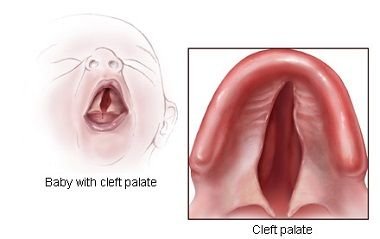
A cleft is a congenital breach in continuity of the face, specifically, the lips, the alveolus or the palate. Clefts occur along planes of the face as a result of defects or faults in the development and maturation of the embryonic processes. Thus developmental defects in the primitive palate, nose and lips result in cleft.
There are various degree of orofacial cleft ranging from simple lip pits or notches to gross bilateral cleft of lip and entire palate, transverse facial clefts, and oblique facial clefts. Clefts occur most times in isolation(Non-syndromic cleft) but in about 20 – 30% of cases they are associated with other malformations or abnormalities which is regarded as syndromic cleft. They are the most common serious congenital anomalies in the orofacial region.
Orofacial clefts are the most common craniofacial birth defects in humans, with an average worldwide prevalence at birth of 1.2 per 1000 births which means in every 2½ minute somewhere in the world, a child is born with an orofacial cleft considering the number of birth per minute that is recorded worldwide.
Orofacial clefts represent a significant public health burden in terms of the immediate and long-term medical costs as well as the social impact on patients and their families. In the United States, for example, the lifetime cost for treating orofacial clefts has been estimated to be approximately $100 000.
Not surprisingly, this birth anomaly is the single most commonly treated craniofacial malformation in a paediatric hospital setting. Although surgery can correct most of the structural defects, patients still face a lifetime of functional, social, and aesthetic challenges.
A little about the history of cleft
Orofacial cleft is as old as the existence of man on earth. Traumatic cleft first mentioned by Celsus in the 1st century. Hippocrates 400BC and Galen 150AD also talked about cleft lip.According to Cockayne (1961), the old English literature book(Bald’s Leech ), which is a compilation of folk medicine produced at Winchester in 950AD, described a form of treatment of harelip as ‘cutting the free edge of hare lip and suturing the wound with silk'.
Garrison(1961) asserted that Jean Yperman, a 14th century surgeon, described a detailed account of the healing of hare lip.
Basky(1964) considered Pierre Franco, a 16th century cleft surgeon as the father of cleft surgery. Franco was recorded as the first to use the word cleft and he published a detailed description of the operation of congenital cleft lip in 1556 & 1561.
{kind=link}
Causes of orofacial cleft
The exact causes of orofacial cleft is unknown however, studies have shown that it could be multifactorial that is a combination of exogenous and endogenous factors (Frazer , 1970).
Possible aetiological factors are:
Endogenous risk factors----- Genetics or Hereditary i.e inherited trait from parents and family members.
Exogenous ------ Environmental factors: These are factors related directly to periods just before or during of pregnancy.
Factors such as Drugs, Hormonal influences, Nutritional deficiencies, viral infections, Irradiation, Increased maternal age, Hypoxia, Consanguinity have been implicated
Who is at risk of having a child with Cleft?
Research has shown that every parent carries a 1 in 700 risk of having a child with cleft.
If a parent have a cleft child,the risk of having another one is 2 -5 %.
If more than 1 person in the immediate family has , risk increases to 10-12%
A child with a cleft has a 2- 5% chances that she will also have a cleft child.
If she has a close relative with cleft too,the risk also increases to 10 – 12%.
The unaffected siblings of a cleft child has the risk of 1% of her child having a cleft
Racial difference
Cleft is more common in Whites (Caucasians) than Negroid
most frequently seen in Orientals / Mongoloid races
Gender - More in males than females,however in cases of isolated cleft palate females are more affected than males. In severe clefts Males are more affected.
U.K 1 in 1000 births, USA 1 : 750 – 900 births
Orientals /Indians 1 in 250 -300 births
Negroes 1 in 2000- 5000 births .
Nigeria 1:2703. America 1:1000
Socio-cultural Issues Associated with Cleft Lip and Palate
Giving birth to a child with orofacial cleft deformities can be particularly distressing causing psychological/emotional distress such as depression for the parents. Contributing to this distressing situation are negative attitude and perception of families and friends as well as even health care providers to this congenital conditions.
The “shame” associated with having a child with this condition has led to killing of these children, or being unable to bring out the children to the outside world. Anecdotal evidence suggests that stigmatization is a common “phenomenon” experienced by families of children afflicted with cleft lip and palate deformities.
This stigma can arise from family members, friends, community members, health care workers, and even the affected parents (internalized stigma). Mothers wanted to abandon the baby in the hospital/place of birth, and also wished the child was never born. Fathers abandoned his wife and all the children after the birth of the affected child
Relatives, friends and neighbours refusal to carry babies born with orofacial cleft.

Problems associated with cleft
Feeding
This is a major problem that a child with cleft, especially cleft that involves the palate(roof of the mouth) usually have because of their inability to create a negative pressure that is needed for sucking. These child battles with failure to thrive as a result of malnutrition. The mother is always advised to feed the child with a special feeding bottle with long teeth or with a cup and spoon after expressing the breast milk.
Hearing
Ear infection (otitis media) is a frequent symptoms usually seen in a child with cleft & if not properly managed can result in permanent loss of hearing.
Speech
Children with cleft of the lip and palate usually find it difficult to pronounce certain words which results in hypernasal speech
Airway problem can also occur especially in those with severe functional & structural anomalies e.g Pierre Robin sequence (micrognathia, cleft palate, glossoptosis)
Dental problems
One of the major problems seen in cleft is nasal deformity which causes poor aesthetic appearance for the child.
others include;
- Missing teeth in both primary and permanent dentition
- Malocclusion: class 111, mandibular prognathism, palatal collapse.
- Associated anomalies such as club foot, neurological disturbances, congenital heart disease and mental retardation which is usually seen in about 30% of all with cleft. However, this is more common in patient with isolated cleft Palate(38%) than in Cleft Lip(21%).
Cancer
Clefts also appear to be associated with a higher risk of cancer in later life and increased overall mortality well into adulthood.
Zhu et al (2002) in a case-control study in Denmark, found no increased risk of cancer in parents having children with malformations in general, but a higher cancer risk in parents of children born with cleft lip/palate
A recent study by Wang et al (2016) in a gene profiling analysis also provided evidence for the linkage between cancer and orofacial cleft.
Certain genes such as SMAD3, PIK3R1, CASP3, TP53 and CDK1, were found to be associated, not only with Non-Syndromic Ceft Lip/Palate, but also with cancer.
Treatment of Clefts
Due to the myriads of problems associated with cleft deformities, the ideal management of cleft lip and palate has been reported as a classic example of a multidisciplinary team approach.The Oral and Maxillofacial Surgeon is an integral member of this cleft team, other members are Plastic Surgeon, Otorlaryngologist, Orthodontist, Pediatrician, Prosthodontist, Speech therapist, Geneticist, Paedodontist, Psychologist, Dental hygienist, and General dental practitioner.
Goal of treatment
- Correction of cleft & associated problems
- Full rehabilitation of patient including social and psychological rehabilitation.
- Objectives: LIP a) Functional----Speech
b) Aesthetics
PALATE: To create a mechanism for a) Speech and b) Deglutition
Surgery is the main stay of treatment of cleft lip and palate and early closure is usually advocated.
Is Intrauterine repair possible?
Due to advancement in technology, diagnosis of cleft,especially cleft involving the lip can be made on ultrasound during pregnancy and in some advanced countries, repair can be done while the babe is still in the womb.This has a lot of advantages as it allows birth of a normal baby thereby preventing psychological /emotional distress for the parents,removes all problems associated with cleft and also allow normal growth of dental arch/maxilla.
Repair can also be done within 48 hours of birth if the infant is generally healthy & of normal weight. This enables mother to take a ‘normal’ child home thereby minimizing feeding problems & embarrassment. However the only obstacle to achieving intrauterine closure is that it requires high-tech equipment, and also its against some cultural belief/practices.
However, in most developing nations, treatment is usually delayed due to lack of equipment and technical-know-how .In such cases,the 'rule of 10' is usually applied for the repair of cleft lip . That is when the baby is 10weeks old, 10lbs in weight, hemoglobin concentration of 10g/dL and 10,000 of White Blood Cell. This is done to allow full comprehensive assessment of child and optimal physical condition for surgery to reduce complications that may occur during surgery.
For palate repair the timing is usually between 6-12 months before speech development starts.

Conclusion
Myths surrounding the aetiology of cleft deformities are prevalent. A well informed public and sensitized professionals are barriers against stigmatization, therefore the public and healthcare professionals must be equipped with necessary knowledge to combat the stigma associated with cleft deformities.
It should also be noted that the management of the child with orofacial cleft involves a breadth that spans multiple disciplines.It could last from infancy to adulthood. Surgical treatments seek to produce lasting form and function that gives adequate consideration to growth and development.
Please note: all pictures used in this post are labelled for free usage.
Thank you for reading.
Being A SteemStem Member
Good write up doc, good to know that oral cleft can be treated.
well done