What is Meckel's Diverticulum? [Topic review + Clinical Case Discussion]
Best regards, dear Steemit community, especially #steemste and #curie, who continually show their support for the medical content I share with you.
On this occasion I wanted to share with you about this interesting topic wich is part of the surgical branch, one that I've always like so much; with the presentation of a clinical case of this pathological entity, in one of my turns in the hospital, at the service of Pediatric Surgery, once again I witnessed that it's not enough to read and study on a specific topic, we always learn much more from the hand of a lived experience.
Since the medical exercise is based not on treating a disease, but on treating the patient; for which the individualization of each patient is so important, to focus on their well-being and recovery; always hand in hand with a knowledge entrenched in the best bibliographies of course. That's why I think that previous the discussion of this clinical case that I had the great opportunity to witness, it's important first to make a small review on the topic of this pathology.

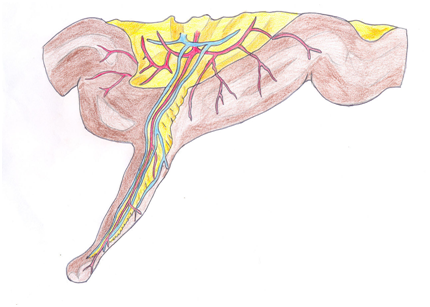
Meckel's diverticulum is part of a group of diseases known as pathologies of the omphalomesenteric duct, which is an anatomical duct that during the early stages of the embryonic period provides vascularization to the yolk sac, and after the development of placental circulation begins to fibrolate from the navel to the intestine (by the sixth week of intrauterine life there should be no connection between the primitive intestine and the abdominal wall). This duct is formed by pluripotential cells, which disappear with their obliteration, however, in some cases they can persist and grow in ectopic or abnormal tissues, such as the gastric or colon mucosa, pancreatic tissue, or duodenal glands. Therefore, the formation of Meckel's diverticulum and other pathologies related to this duct develop as a consequence of an alteration during its embryogenesis.
Meckel's Diverticulum
It's named after the doctor Johann Meckel, who in 1809 first described this defect; wich are sac-shaped evaginations located on the antimesenteric edge of the small intestine; sometimes a portion of heterotopic mucosa (normal tissue with abnormal localization) is also present in Meckel's diverticulum, which leads to possible complications; gastric and pancreatic tissue being the most frequent types, and although the presence of this heterotopic tissue is rare, they're almost always present (especially gastric) in the symptomatic cases of the pathology.
As for the epidemiology, it's the most frequent of all pathologies of the omphalomesenteric duct, and can be present in up to 2% of the population, there's also a certain frequency inclination towards the male genre, with a 4: 1 ratio compared to female.
CLINICAL MANIFESTATIONS:
The clinical picture is diverse, and depends on age of the patient; a mnemonic is often used to describe the main features of the pathology, known as "the 2" rule, which refers to: 2% of the population, less than 2 feet from the ileocecal valve, 2 types of heterotopic mucosa (gastric and pancreatic), patients under 2 years of age, and 2 inches long.
In a considerable percentage of patients with this defect, it's asymptomatic unless it gets complicated; being the main clinical pictures (consequence of complications), hemorrhage, obstruction and inflammation. Hemorrhage and obstruction are very common in children of younger age, compared to inflammatory conditions (these are usually more common in children older than 5 years old). And there are less frequent complications that have been recorded, such as the origin of a neoplasm at the level of the diverticulum, that it's the site of impact of a foreign body, or the development of a parasitic infection.
INFLAMMATION OF MECKEL'S DIVERTICLE:
This being the form of presentation of the clinical case that will be presented below, it seems to me that we should talk about it a little more.
It's a pathology known as diverticulitis and is characterized by being an entity that's rarely diagnosed before surgery; It's a disorder with clinical characteristics very similar to those of an acute appendicitis, in fact when a picture of appendicitis is suspected, but no appendicular anomalies are found, it's essential to carefully examine the intestinal wall for a Meckel diverticulum , since it could be the cause of the symptomatic picture.
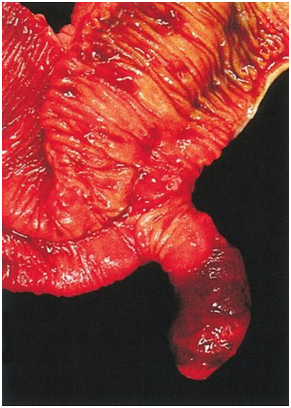
Source: Wikimedia Commons.
The image shows the sample of a Meckel Diverticulum, extracted surgically as a result of an inflammatory process.
Meckel's Diverticulum Surgical Specimen
{kind=link}
The most frequent signs and symptoms include migratory abdominal pain and umbilical redness (Nicola's Sign), product of the spread of inflammation to the abdominal wall when there's a fibrous cord; The presence of both are signs that make us suspect the presence of this pathology.
TREATMENT:
Regarding the performance of an Incidental Diverticulectomy, it's an objective issue of controversy; since the probabilities of whether or not it is counterproductive are evaluated, due to the fact that both the morbidity and mortality derived from the process should be compared with the probability that the diverticulum induces symptoms and subsequently complications.
However, in those symptomatic cases, especially in inflammatory conditions, the surgical approach is essential.

During a guard by the Pediatric Surgery Service I had the opportunity to be invited to observe an operation that had previously been electively scheduled for a different day, the surgery was scheduled to take place within a month or so; It was an 11-month-old male patient who had a history of digestive hemorrhage and where he had the presumptive diagnosis of Meckel's diverticulum.
However, given an acute picture of two days of evolution characterized by abdominal pain of strong intensity expressed through continuous crying and rejection of food, fever quantified at 38.5 ° C, and vomiting in number of 5 and both food and bilious content; it's decided to enter the patient to investigate the cause of the current clinical picture.
Laboratory results are obtained that yield a leukocytosis, with figures of 12,800 xmm3 at the expense of segmented, rest of complete hematology within normal limits; liver enzymes and renal function tests within normal limits in the same way.
Given the clinical suspicion of a possible Meckel diverticulum, due to the history of gastrointestinal bleeding and examinations performed during the first episodes, and the current clinical picture and suggestive laboratory tests, it's decided to surgically intervene in the patient under the diagnosis of Diverticulitis.
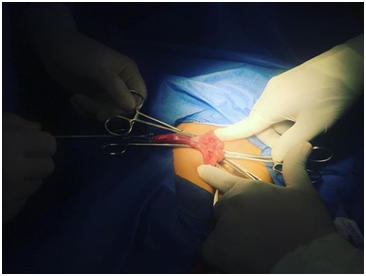

During the surgery a Meckel diverticulum was found approximately 1 foot and 5.7 inches from the ileal-cecal valve, (as mentioned during the discussion of the subject, in most cases the distance between the diverticulum and the valve it's less than 2 feet).
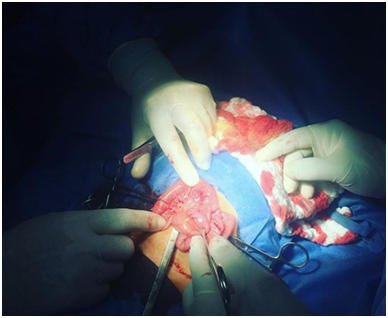
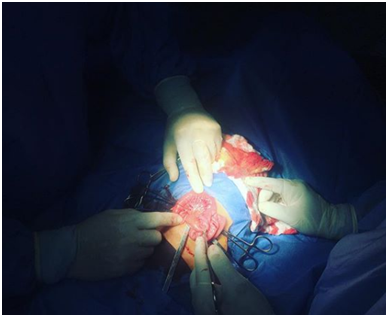
Resection of the diverticulum was performed with two-plane ileal-ileal terminal anastomosis.
And it was decided to carry out in the same way an incidental appendectomy through trans umbilical incision, (since the clinic of both entities is usually very similar as previously explained, and the coexistence of both clinical conditions is not common, but it have been cases reported).
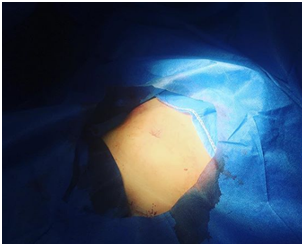
Fortunately, an excellent clinical and aesthetic final result is obtained; the surgical approach is almost imperceptible.
Pending evaluation of the child's post operative evolution.
CONCLUSIONS:
Meckel's diverticulum is a pathology of variable incidence, which is related to an accident or error during embryogenesis of the yolk sac, this under normal conditions should be obliterated and disappear completely in intrauterine life; the permanence of it results in the development of a group of diseases known as pathologies of the omphalomesenteric duct, where Meckel's diverticulum occupies the first place in frequency.
It involves the formation of a group of sac-shaped evaginations located on the antimesenteric edge of the small intestine, at a distance from the ileal-cecal valve that does not exceed 2 feet. Children under two years of age are usually affected symptomatically, since after this age, patients who present with the diverticulum usually evolve subclinically into adulthood, usually without complications.
Among the most common complications are digestive hemorrhages, intestinal obstructions, the inflammatory condition, or the development of neoplasms or infections at the level of the diverticulum.
As explained during the discussion of the topic and the clinical case presented, many times patients can take more than one complication at the same time: such was the case of the described patient, who had presented a history of gastrointestinal bleeding during his short life, and It was subsequently complicated by an inflammatory condition, which is why an emergency intervention was necessary (although inflammation of the diverticulum is usually more frequent in older children, we see how there are always exceptions to the rule).
It's very important to know about this type of surgical pathologies, and its variety of clinical presentations, in order to be able to make a timely and early diagnosis, and thus provide adequate treatment to the patients, to preserve their lifes and health.
BIBLIOGRAPHIC REFERENCES:
[1] Pediatric Surgery - Jesús Fernández.
[2] Pediatric Surgery - Ashcraft & Hollder.
[3] Various presentations of omphalomesenteric duct remnants in children. 12 (J Coll Physicians Surg Pak 2002).
[4] Meckel's Diverticulum: a review. 24 (Clin Anat 2011).
[5] Beltran M, Larenas R. Meckel's diverticulum volvulus: an unusual complication. Chilean Rev. of Surgery. Vol 58-N1, February 2006.
[6] González I, Jiménez S. Diagnosis by CT of intestinal invagination on a Meckel's diverticulum: a case report. Radiology 2001.
[7] Kumar R, Kumar V. Emergency surgery for Meckel diverticulum. World Journal of Emergency Surgery 2008.
- Note: All images of the clinical case are photographs of the author @iradyjr.

Congratulations @iradyjr! You have completed the following achievement on the Steem blockchain and have been rewarded with new badge(s) :
You can view your badges on your Steem Board and compare to others on the Steem Ranking
If you no longer want to receive notifications, reply to this comment with the word
STOPTo support your work, I also upvoted your post!
Vote for @Steemitboard as a witness to get one more award and increased upvotes!
This post has been voted on by the SteemSTEM curation team and voting trail. It is elligible for support from @curie and @minnowbooster.
If you appreciate the work we are doing, then consider supporting our witness @stem.witness. Additional witness support to the curie witness would be appreciated as well.
For additional information please join us on the SteemSTEM discord and to get to know the rest of the community!
Please consider using the steemstem.io app and/or including @steemstem in the list of beneficiaries of this post. This could yield a stronger support from SteemSTEM.