Surgery 3.0: Robotics and Artificial Intelligence
My training as a surgeon is taking place during an extremely “special” period: we are living in the middle of a technological “boom” where automation increase month by month in almost every field. Including medicine.
Soon robotics and artificial intelligence will make surgeons to be obsolete for small surgeries - Image by R. Mirnezami and A. Ahmed.
It is said that surgery is a “dead” discipline because it is believed that there are no more surgical techniques to invento. This brought lots of publications in literature on new techniques that are as “fanciful” as they are useless. For this reason, main research fields in surgery focuses on the refinement of existing techniques and, above all, on the development of new and more advanced tools that can improve surgeon performance and surgery outcomes.
Laparoscopic surgery is the gold standard for almost all kind of surgical procedures due to the low complication rate, the excellent aesthetic results for the patient and its rapid recovery (with a subsequent decrease in hospitalization costs). This method was invented in 1901 by the German surgeon Georg Kelling who “practiced” on dogs: it was only in 1910 that it was first practiced on a patient by the Swedish physician Hans Christian Jacobaeus. At first mocked, this new way of doing surgery soon became widespread all over the world, thanks to new discoveries in the field of anesthesia and the implementation of optical fibers and the new means of hemostasis and dissection.

All laparoscopic procedures generally start with 3 to 5 small skin incisions of about from 0.5 to 1.5 cm. The number depends on several factors, such as the type of surgery and the position of the patient. Through these small incisions few plastic devices that act as accesses to the abdominal cavity called “trocars” are inserted. In order to create workspace, the abdomen is insufflated through the first trocar with carbon dioxide, a non-inflammable gas that could be absorbed by human tissue and it could be removed via respiration: this will raise abdominal wall to make space for laparoscopic instruments. The first trocar is usually used to insert the laparoscopic camera: this will make possible to see where to practice the subsequent incisions that will host other trocars where laparoscopic instruments will be positioned. The main advantages of this method compared to traditional surgery (also called “open technique”) are a reduction of intraoperative blood loss, small skin incisions with a subsequent reduction in infections rate, less pain, fast recovery times and less postoperative complications.
Initially this procedure was considered expensive and difficult to practice. In few year, the technological advancement and the availability of new devices allowed a reduction of procedure costs and an improvement in the overall operating performance: the laparoscopic approach is now considered safe and feasible in almost all abdominal and thoracic surgery.
The new era of surgery aims to minimize the invasiveness of surgery: it seems almost a contradiction considering that the same word “surgery” comes from the Greek cheirourgia (deriving from χείρ, χειρός, hand and ἔργον, work) which indicates a manual work. We are in the era of the minimally invasive surgery and the laparoscopic surgery represents the cornerstone. Anyway, thanks to technology progress, a new surgery technique is being developed: the robot-assisted surgery or RAS. The first RAS was performed in 1983 during an orthopedic procedure by the robot called Arthrobot. However it is in 2009 that the real revolution began, which is when the daVinci Surgical System was launched on the market by the company Intuitive Surgery at the price of 1.75 million of dollars.
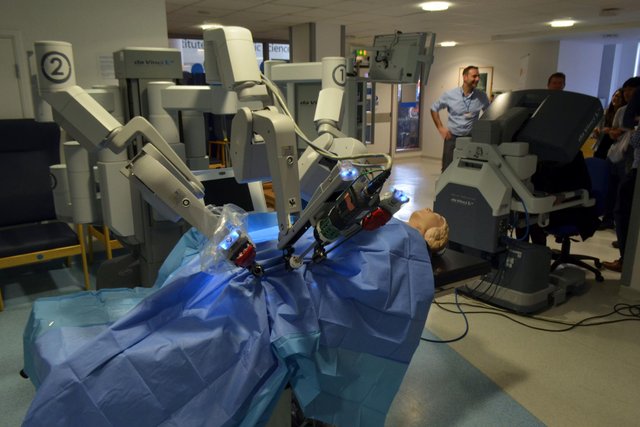
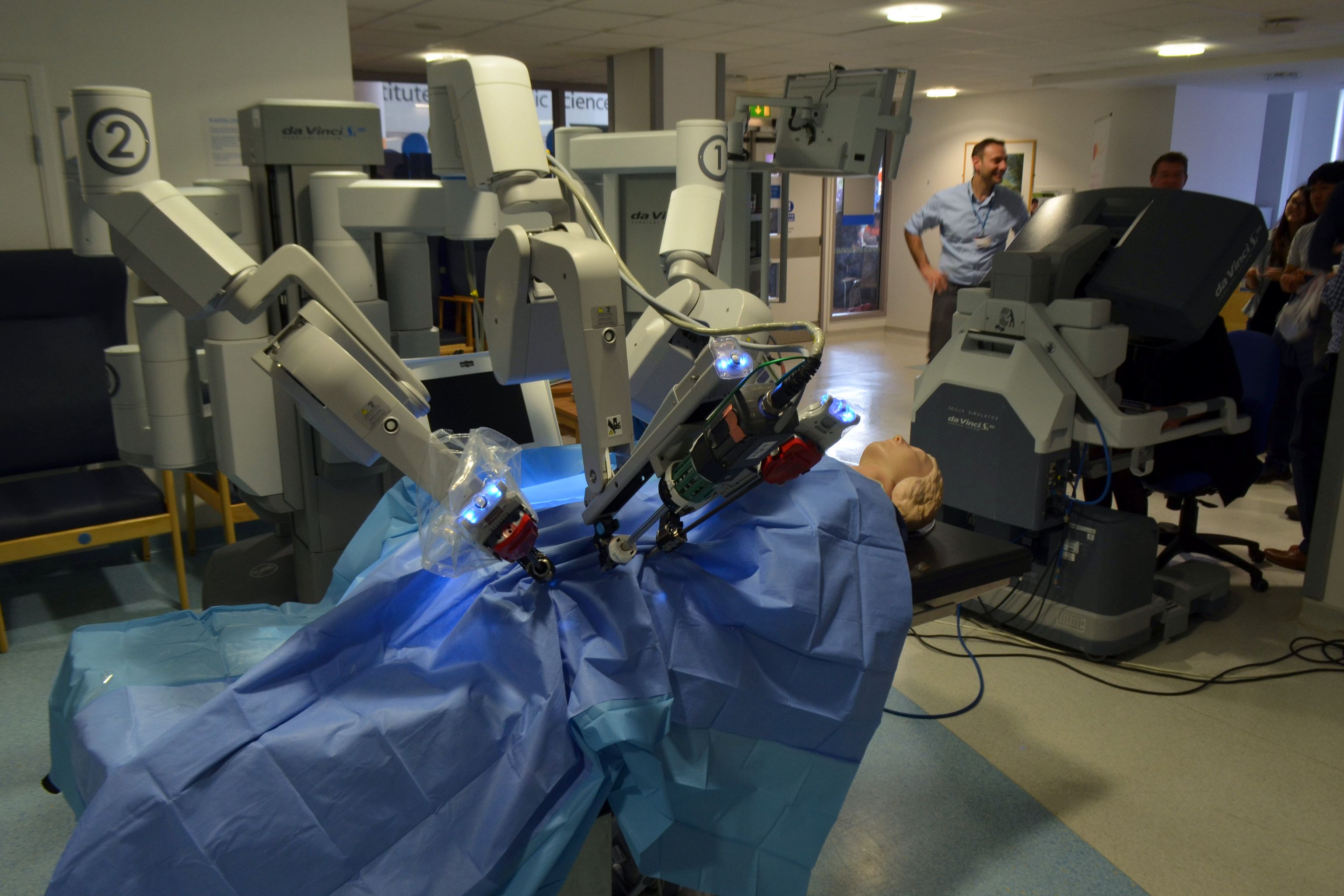
A da Vinci Surgical System at Addenbrooke’s Treatment Centre during the 2015 Cambridge Science Festival – Image of Cmglee – CC BY SA 3.0
The launch of the daVinci was not a great success, as it happened for laparoscopy initially. The reason for this poor success was due to the low cost-efficiency of the machine. In fact, aside from the huge starting cost (about two million of dollars), the daVinci could be used only for an extremely limited number of procedures. Early on it , hospitals used the robotic system mainly as training machinery or as a factor of prestige to flaunt wealth and be counted among the cutting-edge centers. Scientific progress and technological advancement have slightly improved things over time: from the few cardiac and urological procedures the daVinci robot has now its wide field of application and can be used in almost all surgical procedures and, recently, even for organ transplants. Anyway, the diffusion of this technology is heavily limited by the high cost of the robotic system and the skill requirements for the surgeon to effectively use it. Currently, the cost of a “da Vinci” robot system is around $ 1.3 million and each procedure has a cost that ranges between $ 1500- $ 2000 because instruments are one-use.

{kind=link}
{kind=link}
{kind=link}
The daVinci system consists in two main components: the surgeon console and the robot side-cart. The robotic cart consists in several automated arms which have robotic jointed-wrists that can be twisted and rotated exceeding natural human hand movements. The surgical instruments are mounted on the robotic arms and they are inserted into the abdominal cavity through trocars with a procedure that is similar to that of laparoscopic surgery. The surgeon’s console is equipped with a high-definition screen that transmits images of the abdominal cavity coming from the camera mounted on a robotic arm while the control of the robotic arms is done via the “telemanipulators” and two pedals. Through these commands all the surgeon movements are transmitted to the robotic arms with extreme precision. The computerized system is also capable of filtering the surgeon’s involuntary tremors so that they are not transmitted to the robot, making sure that every surgical gesture is perfect. To realize this, take a look at this short video that alone is worth more than 1000 words.
Despite the growing enthusiasm around the RAS, there are still many controversies about its real usefulness. In scientific literature there are several papers reporting discordant results on the performance of the robotic surgery and the war between laparoscopic and robotic surgery fans is still open. In a recent meta-analysis, the group of dr. Hyunsuk Frank Roh showed how robotic surgery did not offer better results in terms of complications, operating times and hospitalization despite having much higher costs than laparoscopic surgery. The only variable that improved was the rate of intraoperative bleeding. However, the meta-analysis of dr. Roh has two important limitations: the first is about the heterogeneity of the collected data in the reviewed publications ( inclusion criteria of patients, surgical techniques and the terminology used). This thing, by the same admission of the authors, can justify the differences from the results of previous meta-analysis. The second limitation is that the experience of the operators has not been taken into consideration in the publications reviewed: this can heavily influences some variables such as the complication rate and the operating times. In fact, experienced robotic surgeons can complete interventions in less time and with less complications. Although this is a young technology, it’s really amazing. The most exciting thing about RAS is that the robotic arms are controlled remotely: one day we can undergo an operation by a surgeon who controls the robotic arms of our operating room being thousands of kilometers away!
While new cheaper (and valid) alternatives to daVinci System are starting some healthy market competition, such as the Senhance Surgical Robotic System and the REVO-I Robot Platform, different groups of engineers, IT and healthcare professionals are developing the first fully automated systems for the operating room. Following the announcement of AlphaZero, the new artificial intelligence capable of self-learning realized by DeepMind (a Google subsidiary), the enthusiasm towards this new type of AI has extended to the field of gaming, cars and lately to the healthcare. Although no one would ever think that a surgeon’s decision-making ability could be replaced by a machine, a first CDS (clinical decision support) for surgery was recently developed. The CDS is an algorithm that can help (actually) the patient’s assessment and it could decide which way to go to improve the outcome of a surgery. Through access to large databases, this algorithm is able to assess and integrate the patient’s personal information, such as biopsy results, radiology, biochemical reports and decide the best therapeutic path to take, even in the surgical field. This algorithm will not only use patient data, but It will integrate them with those of the surgeon’s profile, like surgeon experience and his complication rate, in order to identify which surgeon is the most suitable for that specific procedure on that specific patient.
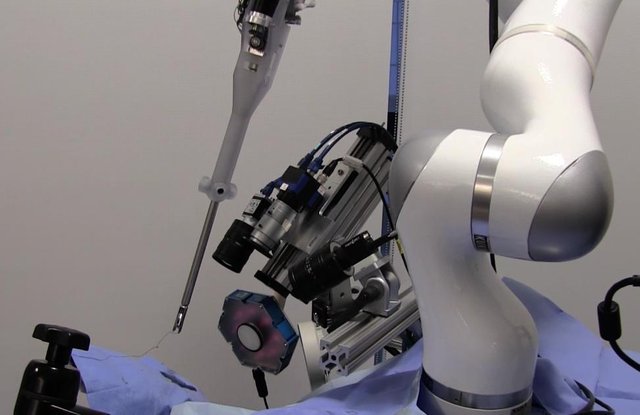
Smart Tissue Autonomous Robot (STAR ). Image by Children’s National Medical Center
However, the real revolution lies in fully automated systems driven by an AI. This is the case of the Smart Tissue Autonomous Robot System (STAR), a robot that is able to sew an anastomosis (connection between two structures, like two loops of intestines) perfectly and overlapping totally the work that would make an expert surgeon. Moreover, in the future small “soft” robots with autonomous functionalities, built with 3D printers, will be able to carry out some stages of the surgical intervention in full automation without any human support. All this post just demonstrates that there is a constant technological evolution, even in the health field where man has always been the master.
The real question here is “to what extent an automatic robot ceases to be a mere tool?”
R. Mirnezami et al. Surgery 3.0, artificial intelligence and the next-generation
surgeon. Br J Surg. 2018 Apr;105(5):463-465. doi: 10.1002/bjs.10860.Roh et al. Robot-assisted laparoscopic surgery versus conventional laparoscopic surgery in randomized controlled trials: A systematic review and meta-analysis. PLoS One. 2018; 13(1): e0191628. Published online 2018 Jan 23. doi: 10.1371/journal.pone.0191628
Finkelstein et al. Open Versus Laparoscopic Versus Robot-Assisted Laparoscopic Prostatectomy: The European and US Experience. Rev Urol. 2010 Winter; 12(1): 35–43.
Rao PP. Robotic surgery: new robots and finally some real competition! World J Urol. 2018 Feb 9. doi: 10.1007/s00345-018-2213-y.
This article is from an own original work published here
This post has been voted on by the SteemSTEM curation team and voting trail in collaboration with @curie.
If you appreciate the work we are doing then consider voting both projects for witness by selecting stem.witness and curie!
For additional information please join us on the SteemSTEM discord and to get to know the rest of the community!
The "Surgery 3.0" really piqued my interest. Having a surgical procedure fully run by AI is the future of medicine; and the future is already here with us.
Maybe in the nearest future, we could behold the rise of complex robo-surgeons.. Now I can imagine how the future would look like.
Nice piece there
Thanks. This future is more close than you ever thing. Robotic surgery just demolished the barrier between human and computers, still there are quite a lot of surgeons that prefer doing things in the old fashioned style.
This post was shared in the Curation Collective Discord community for curators, and upvoted and resteemed by the @c-squared community account after manual review.
Hi @cryptoitaly!
Your post was upvoted by @steem-ua, new Steem dApp, using UserAuthority for algorithmic post curation!
Your UA account score is currently 1.540 which ranks you at #34939 across all Steem accounts.
Your rank has dropped 832 places in the last three days (old rank 34107).
In our last Algorithmic Curation Round, consisting of 302 contributions, your post is ranked at #139.
Evaluation of your UA score:
Feel free to join our @steem-ua Discord server
Really! What an eyeopening post this was for me. I had no idea of any of this!
Thanks!
Ciao @cryptoitaly! Ho provato il DaVinci System l'anno scorso in occasione della giornata della ricerca, c'era la possibilità di fare la simulazione e provare i "test" virtuali per padroneggiare il robot. Nonostante la passione per la tecnologia non è assolutamente intuitivo il controllo secondo me, eppure la precisione dello stesso è davvero elevata. In che chirurgia stai facendo la specializzazione?
si, la settimana prossima sono a Roma al congresso congiunto delle società di chirurgia, sicuramente ci sarà un daVinci con cui giocare un po' :)
The fall of daVinci surgery is never the end. It paved way to the creation/invention of better authometic machines that will enhance the operation of human body.
More than the end, I think it's a starting point. Tech progress will bring us so many new techniques in the future to come!
You are right. These people in tech world are always futuristic.
Wow! Seriously wow!! I knew that technology had advanced in the medical field, but I had no idea it was to this extent! So awesome to see, but your final questions is a good one; and one that I certainly do not have an answer for :)
Thank you so much for sharing @cryptoitaly :)
I'm really glad you enjoyed this post!