Surgery 2.0: beyond human limits
As a young surgeon born in the digital era, I have always been surrounded by technology during my career. If you add to this the deep passion I have for robots, computers and programming, we can explain my excitement when few years ago at the annual meeting of all surgery branches held in Rome, Italy, the “Congresso Congiunto delle Società Scientifiche Italiane di Chirurgia”, I saw my first da Vinci robot and even “played” with it.

Robotic Assisted operating theater - 2016©Intuitive Surgical, Inc - CC BY-SA 3.0
{kind=link}
Surgery is told to be a “dead” field research-wise: there is a little chance that new surgery techniques will ever be discovered and new techniques are more “creative” than useful. For this reason, more than on new techniques, researchers are focused on new device development to assist surgeons and improve surgery outcomes.
A step back: Surgery 1.5
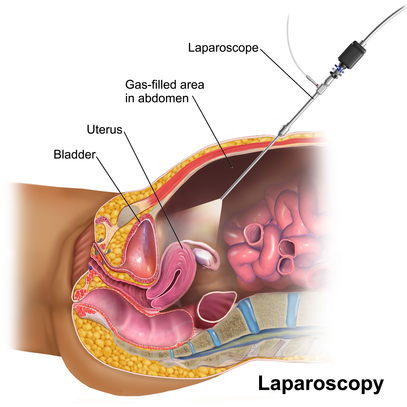
Laparoscopic surgery is actually the gold standard for almost every kind of surgery due to the reduced patient hospital stay, complications rate and improved cosmetic results. Invented in 1901 by a German surgeon named Georg Kelling, it was performed for the first time on humans in 1910 by Hans Christian Jacobaeus, a Swedish internist. Since then, laparoscopy greatly improved thanks to new anesthesia procedures, intraoperatory monitoring, optic fiber and new haemostasis and dissection devices.
{kind=link}
Laparoscopic surgery consists in usually three to five small incisions on abdomen (but the concept is applied also to thoracic or other site surgery) that grant the access to abdomen cavity to rigid endoscopes through ports called “trocars”. Carbon dioxide gas is insufflated in the abdomen to create working space by elevating abdomen wall. Usually there is one endoscopic camera providing on a display high quality images of abdomen cavity while surgeons operate using different endoscopic instruments. The main advantages of this techniques compared to traditional surgery (or “open” surgery) are less blood loss and smaller incisions, which decrease rate of infections, pain, recovery time and grant better scarring process with improved cosmetics. While initially this procedure was costly and high skill demanding, with technology improvements and new devices, laparoscopic surgery is now considered safe and feasible for the majority of abdominal procedures .
But this, was just the “past”.
When engineering meets medicine
New era of surgery aim to further reduce the “body invasion” by the surgeon, with minimally invasive approaches. Here comes into play the Robotic Assisted Surgery (RAS). While first RAS were performed by Arthrobot in 1983 for orthopedic pathologies, the real revolution happened in 2009 when the da Vinci Si Surgical System was launched by Intuitive Surgical on the market, with a price of “only” $1.75 million.[1]
Initially this system had a low distribution mainly for the low cost-efficiency. The huge costs along with the small window of uses made the da Vinci system being a a training tool and a “symbol of progress” for rich hospitals more than something that could be really used. As expected, things went little better over time. While da Vinci system was used initially only for some cardiac and urologic pathologies, its applications extended as surgeons become more proficient and confident with this technology.

da Vinci Xi cart by Intuitive Surgical - CC BY-SA 3.0
Current applications of da Vinci System include:
- Cardiac Surgery
- Colorectal Surgery
- General Surgery
- Gynecologic Surgery
- Head & Neck Surger
- Thoracic Surgery
- Urologic Surgery
- Recently even transplants!
The da Vinci system consists in two components: the surgeon console and the robo-cart, where robotic arms are located. Each robotic arm have a wristed instrument that can bend and rotate more than human hands. These instruments gain access to abdomen cavity via previously placed trocars, exactly like during laparoscopic surgery. The surgeon console has a high definition display that show images captured by the camera placed on a robotic arm; small manipulators called “telemanipulators” are used to control the robotic arms remotely. This way, every surgeon movement is translated to the robotic arms which executes them with extreme precision. Moreover, the computer filters and eliminates all tremors from surgeon hands. Maybe watching this short video will explain it more than 1000 words.
All that glitters is not gold
Despite the growing enthusiasm around RAS, there is still lot of controversy about its use. In literature there are several discordant reports on RAS outcomes and the war between laparoscopic surgery and robotic assisted surgery has no winners right now. Roh et al (2018) showed in a recent systematic review and meta-analysis how RAS, while having higher costs, it has no statistically better treatment outcomes (complication rate, operative time, length of hospital stay) compared to laparoscopy, except the reduced intraoperatory blood loss. [2] The high cost of robotic systems and the high skill requirements make this technology not affordable for all hospitals and limit the diffusion. Currently , da Vinci System costs $1.3 million and each procedure costs $1500-$2000 due to disposable instruments.

da Vinci System remote console - Image under CC0 license
{kind=link}
However, Roh et al meta-analysis has two major limits: the first one is the heterogeneity of data about patients inclusion criteria, surgery techniques and terminology used in the reviewed papers which, according to the Authors , “may contribute to the deviation from previous meta-analyses findings”.
The second one is the lack of information about surgeons proficiency performing robotic assisted procedures, which heavily influences outcomes like operative time, costs and complication rates. As for laparoscopic surgery, robotic assisted surgery has an important learning curve, which differs greatly depending on previous experience. Finkelstein et al (2010) , considering prostatectomy, reported that a surgeon with no experience in laparoscopic surgery need to perform at least 20 robotic assisted procedures in order to gain good proficiency; the number of procedures increase to 60 for an expert laparoscopic surgeon but these numbers can be as high as 200 procedures in order to achieve a good proficiency. [3]
New technologies always have hard time to settle and all the problems described above were probably the same of addressed by first laparoscopic surgeons. Prices of da Vinci System will eventually drop due to the launch of new robot systems and some healthy competition between companies. Proof of this is the recent work of Rao PP. (2018) who compared the da Vinci with two new robotic systems: the Senhance Surgical Robotic System and the REVO-I Robot Platform, both with all the requirements to conquer a piece the market.[4]
Conclusions
The future is exciting and soon we will see high proficiency surgeons being able to perform high skill demanding operations worldwide, without patients need to move themselves, by utilizing remote controlled robots. Development of this technology will also open to new frontiers, like remote controlled micro/nanobots to perform various operations from the inside the human body. [5]Surgery 3.0: still far, but more real than we think.
Follow #steemSTEM tag for more interesting post about science!
References:
da Vinci Si Surgical System. Intuitive Surgical. http://www.davincisurgery.com
Roh et al. Robot-assisted laparoscopic surgery versus conventional laparoscopic surgery in randomized controlled trials: A systematic review and meta-analysis. PLoS One. 2018; 13(1): e0191628. Published online 2018 Jan 23. doi: 10.1371/journal.pone.0191628
Finkelstein et al. Open Versus Laparoscopic Versus Robot-Assisted Laparoscopic Prostatectomy: The European and US Experience. Rev Urol. 2010 Winter; 12(1): 35–43.
Rao PP. Robotic surgery: new robots and finally some real competition! World J Urol. 2018 Feb 9. doi: 10.1007/s00345-018-2213-y.
Robot set loose to film your insides. http://newscientist.com.
Bibliography:
Porpiglia F, Morra I, Lucci Chiarissi M, Manfredi M, Mele F, Grande S, et al. Randomised controlled trial comparing laparoscopic and robot-assisted radical prostatectomy. Eur Urol. 2013;63: 606–14. doi: 10.1016/j.eururo.2012.07.007
Sanchez BR, Mohr CJ, Morton JM, Safadi BY, Alami RS, Curet MJ. Comparison of totally robotic laparoscopic Roux-en-Y gastric bypass and traditional laparoscopic Roux-en-Y gastric bypass. Surg Obes Relat Dis. 2005;1: 549–54. doi: 10.1016/j.soard.2005.08.008
Martinez-Maestre MA, Gambadauro P, Gonzalez-Cejudo C, Torrejon R. Total laparoscopic hysterectomy with and without robotic assistance: a prospective controlled study. Surg Innov. 2014;21: 250–5. doi: 10.1177/1553350613492023
Roh HF, Kim J, Nam SH, Kim JM. Pulmonary resection for patients with multidrug-resistant tuberculosis based on survival outcomes: a systematic review and meta-analysis. Eur J Cardiothorac Surg. 2017;52: 673–8. doi: 10.1093/ejcts/ezx209
Callewaert G, Bosteels J, Housmans S, Verguts J, Van Cleynenbreugel B, Van der Aa F, et al.Laparoscopic versus robotic-assisted sacrocolpopexy for pelvic organ prolapse: a systematic review. Gynecol Surg. 2016;13: 115–23. doi: 10.1007/s10397-016-0930-z
Huang X, Wang L, Zheng X, Wang X. Comparison of perioperative, functional, and oncologic outcomes between standard laparoscopic and robotic-assisted radical prostatectomy: a systemic review and meta-analysis. Surg Endosc. 2017;31: 1045–60. doi: 10.1007/s00464-016-5125-1
Lee SH, Lim S, Kim JH, Lee KY. Robotic versus conventional laparoscopic surgery for rectal cancer: systematic review and meta-analysis. Ann Surg Treat Res. 2015;89: 190–201. doi: 10.4174/astr.2015.89.4.190
Lim S, Kim JH, Baek SJ, Kim SH, Lee SH. Comparison of perioperative and short-term outcomes between robotic and conventional laparoscopic surgery for colonic cancer: a systematic review and meta-analysis. Ann Surg Treat Res. 2016;90: 328–39. doi: 10.4174/astr.2016.90.6.328
Liu H, Lawrie TA, Lu D, Song H, Wang L, Shi G. Robot-assisted surgery in gynaecology. Cochrane Database Syst Rev. 2014: CD011422 doi: 10.1002/14651858.CD011422
Sandoval Salinas C, Gonzalez Rangel AL, Catano Catano JG, Fuentes Pachon JC, Castillo Londono JS. Efficacy of robotic-assisted prostatectomy in localized prostate cancer: a systematic review of clinical trials. Adv Urol. 2013;2013: 105651 doi: 10.1155/2013/105651
Xiong B, Ma L, Zhang C. Robotic versus laparoscopic gastrectomy for gastric cancer: a meta-analysis of short outcomes. Surg Oncol. 2012;21: 274–80. doi: 10.1016/j.suronc.2012.05.004
Asimakopoulos AD, Pereira Fraga C.T., Annino F., Pasqualetti P., Calado A.A., Mugnier C.Randomized comparison between laparoscopic and robot-assisted nerve-sparing radical prostatectomy. Journal of Sexual Medicine. 2011.
I will be featuring it in my weekly #technology curation post for the @minnowsupport project and the Tech Bloggers' Guild! TBG is a new group of Steem tech bloggers and content creators looking to improve the overall quality of the niche.
If you wish not to be featured in the curation post this Saturday, please let me know. Keep up the hard work, and I hope to see you at the Tech Bloggers' Guild!
Thanks a lot! I really appreciate it :)
Interesting post @cryptoitaly. I've resteemed it. I like how robotics and AI are helping out the medical world not just in surgery, but also in diagnostics. I remember there being this diagnostic AI that compares a patient's symptoms to those in a worldwide database. It got much better results than human diagnosticians, especially for the more rare diseases out there.
Thanks a lot! Medicine and technology are deeply connected, as surgeon I look forward new tools for either diagnosis and surgery! :)
You got a 16.89% upvote from @mercurybot courtesy of @cryptoitaly!
Congratulations! This post has been upvoted from the communal account, @minnowsupport, by Weltall from the Minnow Support Project. It's a witness project run by aggroed, ausbitbank, teamsteem, theprophet0, someguy123, neoxian, followbtcnews, and netuoso. The goal is to help Steemit grow by supporting Minnows. Please find us at the Peace, Abundance, and Liberty Network (PALnet) Discord Channel. It's a completely public and open space to all members of the Steemit community who voluntarily choose to be there.
If you would like to delegate to the Minnow Support Project you can do so by clicking on the following links: 50SP, 100SP, 250SP, 500SP, 1000SP, 5000SP.
Be sure to leave at least 50SP undelegated on your account.
You got a 25.53% upvote from @inciter courtesy of @cryptoitaly!