Medical utility of Intraosseous Infusion
On many occasions, channeling to a peripheral route is impossible, especially at extreme ages when you are suffering from severe dehydration or extensive burns. Today the present technique, which despite not being very common and is considered a last resort, is important to take into account and know about it.
Intraosseous lines are an alternative for administering electrolyte solutions, drugs and blood products such as blood into the body. This technique, which had been forgotten, was taken up again in the 80s, as a need to obtain a permeable vascular access for everyone of pediatric age during cardiopulmonary resuscitation.
However, this procedure is only 17% successful and several studies show that the peripheral route is still the ideal, safe and fast method, with the central routes taking second place. The estimated time to channel an intraosseous line is about 5 minutes compared to the central line of 9 minutes.
Intraosseous infusion is fast, safe and effective especially in neonates in intensive care, and adults where channeling a peripheral or central line is almost non-existent.

Public domain Pixnio
Anatomy and physiopathology
In our body the long bones are made up of a dense and firm outer crust, with a light interior called the cancellous bone or spongy portion. There is a network of nourishing arteries that supply the bone with its vascularization.
At the level of the long bone bark this arterial network of nutrients perforates and crosses dividing into ascending and descending branches that later are subdivided into arterioles and capillaries. While the venous drainage derives from the capillaries that lead to the interior of the venous medullary sinusoids, located at the ends of the long bones, that is, the distal and proximal portion, thus flowing through the central venous channel.
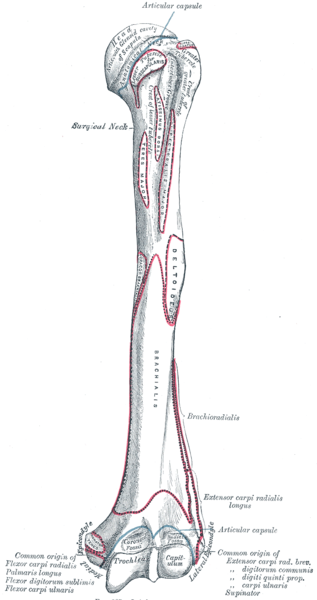
Left humerus. Public domain CC BY-SA 3.0
It is for this reason that the intraosseous needle is inserted through the cortex into the bone marrow of the long bones. Several anatomical areas can be used to access the marrow portion. The safest and most common area to channel an intraosseous line in pediatric patients is the anteromedial surface of the proximal tibia. While the distal portion, above the medial malleolus, is the most commonly used area in the adult. A third option to achieve an intraosseous access is the anterior surface of the distal femur.
It is very important to remember that drugs and solutions administered by intraosseous route will immediately reach the systemic circulation.
Indications
The placement of an intraosseous line is indicated when a vascular access is urgently needed for the resuscitation of a patient and it fails to channel a usual line. This technique has been used mainly for the paediatric population in situations of cardiac arrest, but has also been useful in adults.
There are situations that may require the placement of an intraosseous line, such as: cardiac arrest, shock, trauma, severe dehydration, extensive burns, epileptic status or any other situation that urgently requires the administration of drugs or fluid therapy.

In addition to being useful for medication administration, blood can also be drawn and ABO group checked, cross-checked, and other laboratory tests performed. Electrolyte, creatinine, urea, glucose, calcium, and blood gas values are similar to those obtained from samples taken from peripheral or central lines.
Contraindications
In cases of bone disease, and osteoporosis. Avoid placement through areas where skin and tissue infections, such as cellulite or abscesses, are evident. Fractures in the ipsilateral bone increase the risk of compartment syndrome due to extravasation. Failure to place an intraosseous line in the same bone is a relative contraindication.
Medications and fluids that can be given intraosseusly
Medications: adenosine, antibiotics, anesthetics, atropine, calcium gluconate, counting media, dexamethasone, diazepam, digoxin, dobutamine, dopamine, ephedrine, epinephrine, heparins, insulin, lorazepam, morphine, naloxone, phenobarbital propanolol, phenytoin, among others.
Fluids: dextrose solutions, sodium chloride solutions, lactated ringer, globular concentrate, plasma and other blood derivatives.
Materials

Jamshidi Needle. Public domain CC BY-SA 3.0
Intraosseous needles come in various sizes and styles including, Cook intraosseous needle, Illinois sternal/iliac aspiration needle, Sternal/iliac aspiration Jamshidi needle. These needles consist of a detachable handle, an intraosseous needle, a punch, and a safety sleeve to prevent the needle from over-penetrating and causing injury. These needles are between 12 and 20 gauge.
Specific intraosseous needles have been designed for this procedure. Currently, a new intraosseous sternal infusion device has been developed, which consists of a multi-component system to be used in sternal intraosseous accesses in adults. However, it has not been fully accepted by all health communities because of its somewhat higher risk of complications such as deep penetration injury to the heart, lung and mediastinum.
Method
As usual, the patient or representative should be informed of the procedure to be performed, with its risks and benefits. To begin, the patient should be placed in a supine position with the lower limb held behind the knee with a towel. Identify through palpation the anatomical references needed for the procedure.
The frequent area of choice is usually the proximal tibia, and alternatively the distal portion of the tibia or femur. We should palpate the anatomical references in the case of the proximal tibia such as the tuberosity and the anthero-medial surface of the tibia. The bone references in the case of the distal tibia are at the junction of the medial malleolus and the anteromedial surface, posterior to the great saphenous vein.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
In relation to the reference point if the portion to be used in the distal femur, the lateral and medial condyles are taken into account, the femur and the patella. The intraosseous needle should be placed about 2 centimeters above these structures, however, this area is not very useful since the presence of muscle and tissue structures is abundant.
Once the desired portion is located, asepsis and antisepsis measures are performed on the skin with povidone-iodine solution. Performing this procedure is very painful for the patient, so the use of local anesthetic is recommended. Local anesthetic is infiltrated into the skin, subcutaneous cellular tissue and the periosteum located over the site where the bone puncture will be performed.
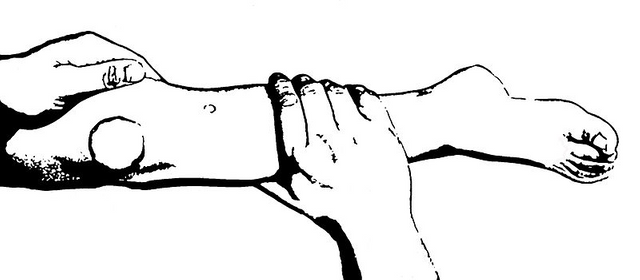
Having clearly identified the area where the puncture will be carried out for the intraosseous infusion, it is necessary to examine that the intraosseous water is functional, re-identify the anatomical references with the non-dominant hand, and stabilize the extremity with the non-dominant hand.
{kind=link}
Pediatric leg for identification of proximal tibeal intraosseous insertion site landmark. Public domain CC BY-SA 3.0
Holding the water firmly with the dominant hand, and the handle of the needle held tightly by the dominant hand, insert the needle perpendicularly or at a slight angle. Use caution as the needle should always be kept away from the growth plate to avoid damage to it.
Direct the needle in a caudal direction in the case of the proximal tibia and in a cephalic position in the case of the distal tibia.
Proceed to advance the needle through the skin and subcutaneous tissue to the bone and insert, during the act of may use a rotary or circular motion to puncture the bone cortex. When the cortex is perforated and the needle enters the medullary cavity, the resistance with the passage of the needle is reduced, so the index finger is used 1 cm above the edge of the needle before the advance as this will avoid excess perforation. Needle advance should be stopped when the medullary cavity is reached.
Remove the perforation when the medullary cavity is reached, attach the 5 0 10 ml syringe to the centre of the intraosseous needle, and aspirate blood, thus confirming that the insertion of the needle is correct.
Finally, attach the intravenous system to the centre of the needle and start the infusion of drugs or solutions required.
Check
To determine that the insertion of the needle was correct, aspirate blood from the medullary cavity and thus corroborate its good location. A second option to know if the location of the needle is adequate, observe if the needle is kept upright without being held. It may also be useful to use a portable fluoroscopy device to confirm the correct placement of the intraosseous needle.
After care
Once the duct is channelled, the intraosseous needle must be secured by means of fixation, and the limb where the puncture was taken must be immobilised. From the immobilization, it is recommended to remove the intraosseous line once the desired drugs have been administered and channel a peripheral or central line as soon as possible.
Complications
The most frequent complications are subcutaneous and subperiosteal fluid extravasation due to difficulties during the execution of the technique. On the other hand, cases of fractures have been described, mainly of the tibia, secondary to excessive penetration of the bone cortex.
A compartment syndrome may be generated when extravasation occurs or when intraosseous lines are placed in fractured bones, as well as skin and tissue necrosis underlying the puncture by drug or fluid extravasation.
Localized infections such as cellulite or subcutaneous abscesses can also occur.
Sources:

steemSTEM is a project of the chain of blocks that supports the scientific content in different areas of science. If you want to know more about this wonderful project you can join the server in discord
This article will be published at https://www.steemstem.io/
link
If you have any questions about any topic of medicine or present any disease you can comment the publication or write me in discord and I will attend you.
Dr. Ana EstradaI hope you enjoyed my content.
Congratulations @anaestrada12! You have completed the following achievement on the Steem blockchain and have been rewarded with new badge(s) :
You can view your badges on your Steem Board and compare to others on the Steem Ranking
If you no longer want to receive notifications, reply to this comment with the word
STOPTo support your work, I also upvoted your post!
Vote for @Steemitboard as a witness to get one more award and increased upvotes!
This post has been voted on by the SteemSTEM curation team and voting trail. It is elligible for support from @curie and @minnowbooster.
If you appreciate the work we are doing, then consider supporting our witness @stem.witness. Additional witness support to the curie witness would be appreciated as well.
For additional information please join us on the SteemSTEM discord and to get to know the rest of the community!
Thanks for having used the steemstem.io app and included @steemstem in the list of beneficiaries of this post. This granted you a stronger support from SteemSTEM.
Thank you very much @steemstem
Hello,
Your post has been manually curated by a @stem.curate curator.
We are dedicated to supporting great content, like yours on the STEMGeeks tribe.
If you like what we are doing, please show your support as well by following our Steem Auto curation trail.
Please join us on discord.
Thanks @stem.curate
Finally some emergency medicine topics! Wonderful!
Thank you, I hope this content can be of help to some people. I just published a new post you can read it if you like emergency medicine topics