The War of the Salt: Guilty or Innocent? / La guerra de la sal: ¿culpable o inocente?

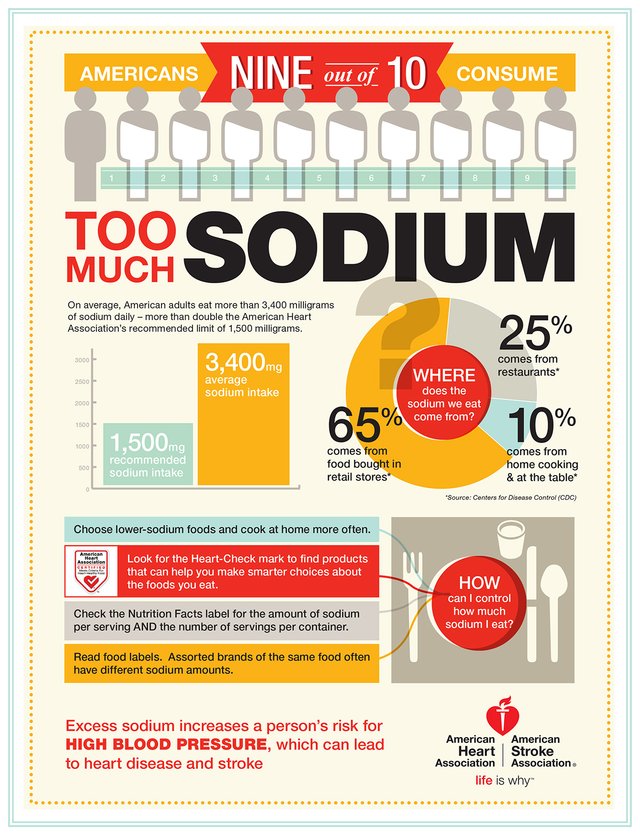
What is the severity of the problem:
INTRODUCCION
La Hipertensión Arterial es unas de las principales causas de morbi mortalidad en la población mundial, actualmente se han realizado grandes avances en el conocimiento de su fisiopatología y tratamiento mejorando el pronóstico y complicaciones de nuestros pacientes, sin embargo por décadas se ha relacionado el consumo de sal con el etiología, mal control y complicaciones asociadas a la HTA, realizando una revisión de las últimas publicaciones vemos muchas controversia en la influencia del alto consumo de sal en la hipertensión Arterial, ¿Pero realmente cual es la relación entre la sal y la HTA? O Todos los Hipertensos son sensibles al consumo de Sal?.
Actualmente surge un concepto que cada vez toma más vigencia como son los pacientes “Sodio Sensibles”, que aclara un poco cuales paciente hay que hacer una restricción más rigurosa en la ingesta de sal y quienes no, sin embargo para nadie es un secreto que la industrialización y comercialización de los alimentos, ha tenido fuerte impacto en el consumo de sal, quienes durante siglos van incrementando las concentraciones de Sodio en los alimentos con la intención de aumento su consumos e ingresos.
INTRODUCTION
Arterial Hypertension is one of the main causes of morbidity and mortality in the world population, currently there have been great advances in the knowledge of its pathophysiology and treatment, improving the prognosis and complications of our patients, however for decades the consumption of salt with the etiology, poor control and complications associated with HBP, making a review of the latest publications we see many controversies in the influence of high salt intake in arterial hypertension, but what is really the relationship between salt and HBP? Or are all patients sensitive to salt intake?
At the moment a concept arises that every time takes more validity as they are the patients "Sensitive Sodium", that clarifies a little which patient there is to do a more rigorous restriction in the salt intake and those who do not, nevertheless for nobody it is a secret that the industrialization and commercialization of food, has had a strong impact on the consumption of salt, who for centuries are increasing the concentrations of sodium in food with the intention of increasing their consumption and income.
Humans currently consume much more salt than for which the species may be evolutionarily suited. It has been theorized that Paleolithic man consumed approximately 0.69 g of sodium per day. In comparison, the average present day human consumes approximately 4.9 g of sodium per day.
How Did the Controversy Appear?

Links
This discordance between present day salt intake and what the human species is genetically programmed to handle has been theorized to have led to the phenomenon of essential hypertension. Proponents of this theory cite the fact that hypertension is not found in societies consuming a “traditional” diet with minimal salt intake. In the 1960’s Dahl observed that hypertension was not present in a sample population of Alaskan Inuit, who ingested a mean of 1.6 g of sodium per day, whereas hypertension affected 8.6% of an American sample, who ingested a mean of 3.9 g per day.
Later, the larger INTERSALT database supported this association. INTERSALT was an observational study of 10,079 men and women aged 20-59, randomly sampled from 52 centers from around the world. Sodium intake was estimated from 24-hour urine collections. The population with the lowest median blood pressure of 95/61 mmHg was the Amazonian Yanomamo Indians who also had the lowest observed median sodium intake of 0.0046 g per day. Blood pressure was then observed to increase, albeit with significant inter-group variability, in populations with higher sodium intakes.
For example, the sample of urban Canadians ingested 3.3 g of salt per day and had a median blood pressure of 119/73, whereas the South Korean sample ingested over 4.6 of sodium per day but only had an associated blood pressure of 109/71 mmHg. Data from the recent Prospective Urban Rural Epidemiology (PURE) study involving over 100,000 individuals from 18 countries also supported a significant association between daily salt intake and increases in both diastolic and systolic blood pressures. These researchers found a 2.11/0.78 mmHg increase in blood pressure for each 1-g increment in estimated sodium intake. While, the observational data from both PURE and INTERSALT do not prove a causative link between salt intake and blood pressure, they are suggestive.
Whereas the above population studies could be confounded by differences in genetics between groups, a further piece of supporting evidence is provided by studies showing increased blood pressure and sodium intakes in urban migrants compared to rural controls of the same ethnicity. Finally, and of greatest empirical weight, there have been numerous interventional trials for the effect of a low or high salt diet on blood pressure. A recent meta-analysis of these trials found that systolic blood pressure was reduced by 3.5/1.8 mmHg on a low- versus highsalt diet. One of the strongest trials was a double-blind randomized crossover trial in 20 humans with untreated mild essential hypertension. In this study mean blood pressure was 147/91 mmHg on 1.2 g of sodium per day compared to 163/100 mmHg on 4.8 g per day.
Physiologic mechanisms of sodium excretion
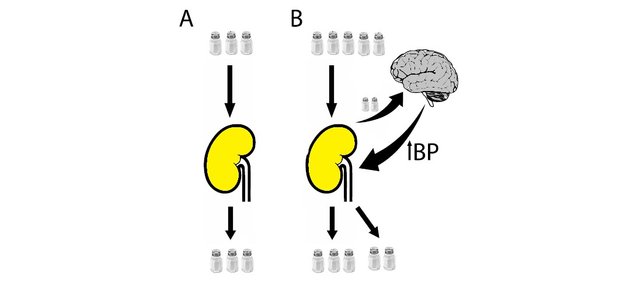
The new paradigm that is developing is that a sodium load in the context of the complex interaction
- Effective excretion of the sodium load with no impact on BP
- Sodium buffering in the “third compartment” with appropriate signals (the dendritic cell-TONEBP-VEGF-C axis) assuring that this is not accompanied by a BP increase.
- Sodium retention without effective excretion or buffering of the sodium load and a BP increase with detrimental consequences.
How does the body sense excess salt and raise blood pressure? Early theories centered on increased plasma volume: sodium retention was thought to lead to increased serum sodium leading to increased thirst and plasma volume. This would then result in increased cardiac index and increased blood pressure. However, while cardiac index may initially rise in the setting of salt loading, this will usually return to normal while total peripheral resistance (TPR) will rise and remain elevated, at least in the hypertensive elderly. Furthermore, plasma volume is inversely related to blood pressure in patients with chronic hypertension (17). Finally, in a study comparing hemodynamics between normotensive and hypertensive individuals, cardiac index was similar while TPR was significantly elevated. Hence, it seems that the blood pressure rise in chronic salt loading is the consequence of peripheral vascular constriction with other hemodynamic parameters remaining constant.
RISK FACTORS FOR SALT INDUCED HYPERTENSION
In the face of increased sodium intake, some individuals will maintain constant blood pressure while others will demonstrate salt-sensitivity and an increase in mean arterial pressure. This phenomenon may explain the wide variation in dietary salt to blood pressure response in observational and salt loading trials. In fact, one interventional salt loading study in healthy normotensive male volunteers found individual blood pressure increases ranging from 1.5% to 34%.
PREVENTION: KNOWING FOODS HIGH IN SALT

7 Salt Myths

RECOMMENDATIONS

{kind=link}
CONCLUSIONS
It is important to be cognizant of evolutionary history. Essential hypertension may be the result of a human maladaptation to an increase in dietary salt intake and a decrease in dietary potassium intake that are recent on an evolutionary time scale. When renal sodium mechanisms are overwhelmed, the body responds by raising blood pressure to enhance urinary sodium excretion.
However, this becomes maladaptive in the long run by increasing the risk of cardiovascular disease. Any physiologic state that reduces urinary sodium concentrating ability such as CKD, aging, African descent or a low potassium diet will increase an individual’s risk for salt induced hypertension. Due to the above considerations, any successful, long-term treatment of hypertension will likely need to induce natriuresis. It is acknowledged that many of these statements remain theoretical. In particular, research remains to determine whether hypertension indeed enhances urinary sodium concentrating ability in humans.
Three Basic Aspects to be examined:
1.-Important to perform a complete diagnosis of hypertension with support of complementary studies (echocardiogram, ambulatory monitoring of blood pressure)
2.- Perform Determination of Sodium and Urinary Potassium concentrations.
3.- Complete study of genetic susceptibility in HBP (Etiology and Treatment)
Taking into account these 3 basic aspects, we can define who of the patients really needs a reduced intake in salt, and thus individualize the treatment for each patient guaranteeing its effectiveness.
CONCLUSIONES:
La hipertensión esencial puede ser el resultado de una mala adaptación humana a un aumento en el consumo de sal en la dieta y una disminución en la ingesta de potasio en la dieta que son recientes en una escala evolutiva. Cuando los mecanismos renales de sodio son aumentados, el cuerpo responde aumentando la presión sanguínea para mejorar la excreción urinaria de sodio. Sin embargo, esto se convierte en una mala adaptación a largo plazo al aumentar el riesgo de enfermedad cardiovascular. Cualquier estado fisiológico que reduzca la capacidad de concentración de sodio en la orina, como la ERC, el envejecimiento, la ascendencia africana o una dieta baja en potasio, aumentará el riesgo de hipertensión inducida por la sal.
Debido a las consideraciones anteriores, cualquier tratamiento exitoso a largo plazo de la hipertensión probablemente necesite inducir natriuresis. Se reconoce que muchas de estas declaraciones siguen siendo teóricas. En particular, la investigación permanece para determinar si la hipertensión de hecho mejora la capacidad de concentración de sodio urinario en los humanos
Tres Aspectos Básicos a considerar:
1.-Importante realizar un Diagnóstico completo de HTA con apoyo de estudios complementarios (Ecocardiograma, monitoreo ambulatorio de presión arterial)
2.- Realizar Determinación de concentraciones de Sodio y Potasio Urinario.
3.- Estudio completo de susceptibilidad genética en HTA (Etiología y Tratamiento)
Teniendo en cuenta estos 3 aspectos básicos, podemos definir quien de los pacientes realmente necesita una ingesta disminuida en sal, y así individualizar el tratamiento para cada paciente garantizando su efectividad.
References
James J. Di Nicolantonio, y otros (2017). The History of the Salt Wars, The American Journal of Medicine (2017) 130, 1011-1014.
Michael A. Garfinkle y otros (2017). Salt and Essential Hypertension: Pathophysiology and Implications for Treatment, Journal of the American Society of Hypertension (2017).
Branko Braam y otros (2017). Understanding the Two Faces of Low-Salt Intake, Curr Hypertens Rep (2017) 19:49.
American Heart Association (2017).Sodium and Salt [Portal Web en Línea]. Recuperado de: http://www.heart.org/HEARTORG/HealthyLiving/HealthyEating/Nutrition/Sodium-and-Salt_UCM_303290_Article.jsp#.WycweaczaM-
good article
Thank you very much for the contribution
Muchas Gracias, nos impulsa a seguir adelante
Congratulations @alfonzoasdrubal! You have completed some achievement on Steemit and have been rewarded with new badge(s) :
Click on the badge to view your Board of Honor.
If you no longer want to receive notifications, reply to this comment with the word
STOPDo not miss the last post from @steemitboard!
Participate in the SteemitBoard World Cup Contest!
Collect World Cup badges and win free SBD
Support the Gold Sponsors of the contest: @good-karma and @lukestokes
Congratulations! This post has been upvoted from the communal account, @minnowsupport, by alfonzoasdrubal from the Minnow Support Project. It's a witness project run by aggroed, ausbitbank, teamsteem, theprophet0, someguy123, neoxian, followbtcnews, and netuoso. The goal is to help Steemit grow by supporting Minnows. Please find us at the Peace, Abundance, and Liberty Network (PALnet) Discord Channel. It's a completely public and open space to all members of the Steemit community who voluntarily choose to be there.
If you would like to delegate to the Minnow Support Project you can do so by clicking on the following links: 50SP, 100SP, 250SP, 500SP, 1000SP, 5000SP.
Be sure to leave at least 50SP undelegated on your account.
It appears you have exposed your private MEMO key as a memo in a recent transfer.
We suggest changing your password before another user can maliciously use it; reading any encrypted messages sent to your account, or pretending to be you on services such as Minnow Booster.
To change your password go to https://steemit.com/submit.html and fill out the form.
It appears you have exposed your private MEMO key as a memo in a recent transfer.
We suggest changing your password before another user can maliciously use it; reading any encrypted messages sent to your account, or pretending to be you on services such as Minnow Booster.
To change your password go to https://steemit.com/change_password and fill out the form.
This post has received a 15.5 % upvote from @boomerang.
This post has received a 9.75 % upvote from @booster thanks to: @alfonzoasdrubal.