Medical Microbiology, Spirochaetes and Syphilis / Microbiologia medica, Spirochete e Sifilide
Spirochaetes
Spirochaetes are very important from a medical and pathological point of view because they cause diseases of a certain severity, many times even fatal.
One of these, sadly known, caused by a species called Treponema Pallidum Pallidum, is syphilis.
General characteristics of spirochaetes
Gram negative bacteria
Very mobile due to the presence of scourges inside the outer membrane, for this reason called endoflagels which make them move almost like snakes. These organelles provide them with a spiral or small spring shape and hence the name of spirochaetes.
Size: considerable length but reduced thickness (< 0,5 micrometers), bacillus shape or better spiral.
Not easily visible with the optical microscope, so a microscope is used in the dark field, and can not be detected with a coloring of Gram, but are needed more complex colors.
.Diagnosing these bacteria is quite complex both in terms of isolation, staining and even indirect diagnosis of their presence through the formation of antibodies.
Normally they are pathogenic and cause serious madness in humans, in many cases, however, the spirochaetes are commensal of many organisms. For example: spirochaetes in the oral cavity of humans that participate in forming that microbial biofilm that is the basis on which the commensal bacterial flora is formed.
Most of these bacteria arrive occasionally in the blood through tooth brushing, giving immune reactions although they are part of the body's own flora, and these reactions interfere when a serological diagnosis of these diseases, in particular syphilis, is made.
There are three main genera that belong to the family of spirochaetes:
- Borrelia = capable of giving even serious infections and autoimmune diseases;
- Leptospira = Frequent in the Po Valley areas due to the high presence of rodents, it can be fatal;
- Triponema = is the most problematic genus and produces the syphilis strain, which is now clearly increasing in our countries, so it is important to take into account its severity.

Syphilis
The disease is widespread throughout the world and is serious.
The bacterium that causes this disease is the Treponema Pallidum of the subspecies Pallidum (full name in the cataloguing is Treponema Pallidum Pallidum), it is a classic spirochaete with spiral or molletine shape, it is a negative Gram and man is the only recognized host (it is not a zoonosis that can be contracted by other animals, it is transmitted only from man to man).
Isolation
Until recently, it was cultivated in particularly susceptible animals such as rabbits, particularly in the testicles. Once inoculated in this district, the bacterium manages to grow in considerable quantities giving swelling of the testicular sac, the biological liquid taken from the testis gives rise to billions and billions of live and dangerous bacteria. So this is the only way to isolate them.
Today it is no longer practiced for reasons related to the health of rabbits and also to that of man, in fact with the method just described were high the chances of infection to the detriment of laboratory technicians. This disease is contracted only by contact, if the areas of the skin exposed to the bacterium have lesions, because the bacterium being very thin is able to pass through even very small wounds of the skin and give syphilis infection. Because of its thinness, even though it is a negative Gram, it does not stain with the typical colour of this class of bacteria.
You can see it alive and you can appreciate its movements under the microscope in the dark field. It is not the classic one with the slide, but there is a small black glass depression in the object holder where a drop of the sample is deposited.
The concept on which this microscope is based is similar to that of the night sky, we are in the dark part of the Earth, the Sun stands behind us and the Moon reflects the light of the Sun, not its own, making itself visible from the Earth. The reflection of the polychromatic light appears white to us, being the set of ghosts.
This same light is the one we see with bacteria when placed in the cell and illuminated, not from below, but from the side, the glass lets the light pass through and what returns to us is the reflected light of bacteria. Together with the reflected light we can see the motility of these microorganisms that are spiral and how snakes move very fast in the liquid
Nelson's Neutralisation Test
In the past, this motility was used for a neutralisation test, called Nelson's test, which aimed to see if there were antibodies in the human body capable of blocking these bacteria and thus neutralising their pathogenetic activity. The procedure involved using a darkfield microscope and adding a drop of patient serum to the Treponema Pallidum bacterium.
If one observed the formation of aggregated clusters that were no longer functional, these indicated that the patient had developed neutralizing antibodies and that he could therefore undergo spontaneous healing of the disease. Today the dark field has been abolished both for the visualization of the bacterium and for the carrying out of Nelson's test, because of the high danger. Many technicians have only become infected with syphilis by manipulating biological samples or by working with vital material.
Subjects most exposed to the disease
Mainly it is a disease that is sexually transmitted, syphilis today is expanding rapidly even in Europe where it had had a blockade between the years 60-70, is again exploding among young people because it commonly contracts with sexual intercourse. The most affected:
Sex workers, homosexuals
In general, anyone who has sex is at risk (endemic among sex practicers).
those who use illegal drugs and drugs
It can also be transmitted through a simple kiss without sex, this practice is called petting.
Those who undergo blood transfusion, but with the procedures and controls that are carried out today in developed countries, nothing should happen.
Who is in contact with the bacterium, for example with the accidental direct inoculation of the blood bacterium in laboratories?
.It can be said that whatever you do that involves the exchange of blood, saliva, biological fluids, manipulation of the bacterium frequently can cause infection. The bacterium also passes from the mother to the fetus during gestation or to the newborn during a natural birth. Often the infection in the uterus leads to the death of the fetus. The birth of an infected infant in the uterus or at birth leads to significant mental retardation and various malformations. In these conditions, only if we do not know the history of the pregnant woman would we proceed to a natural birth, which is risky, otherwise we would have a caesarean section. In the field of embryogenesis until the development of the fetus sees this being susceptible to a very serious infection by Treponema Pallidum Pallidum.
Stages of the disease
Syphilis has several stages, the last of which is fatal, but it is in the first and second that there are many bacteria in the infected body and that it is therefore infectious for the people around it. Today it is believed that the sweat of these people is also infectious, so everything they touch and clothing are possible vehicles of the disease.
Both in the primary and secondary phase the patient is highly infectious, in these phases the active lesions can be on the lips, in the oral cavity, on the genitals, or in the areas that sexually speaking can be of easy exchange of infected material. Once, during the secondary phase, the bacterium enters the bloodstream it is able to go all over the body and reach the central nervous system creating a multi-organ infection that manifests itself with striking symptoms not easily confused with other pathologies.
It is a chronic disease, slowly progressive, and that does not manifest itself clearly at once, the tertiary phase arrives only after 10-20 years as AIDS, during this period of latency the patient is still infectious. While the second stage arrives immediately after the first and therefore the disease is fast, after the second stage there is a latency period that can be more or less long and it is the moment in which it is understood if the patient has managed to heal, if he has managed to control the disease, but not to eradicate it becoming, therefore, a healthy carrier or if it goes against the tertiary, final and fatal phase. Each phase presents unique phenomena and symptoms and from a practical point of view it is unmistakable.
Primary phase (6 days-1 month)
The first phase, also known as "canceride", begins with a vesicle full of liquid that manifests itself at the inoculation point of the bacterium, i.e. where it found the lesion and entered the mucous membrane, and begins to proliferate in the dermis. Replication gives rise to a form of vesicle that can evolve into an ulcer full of Treponema Pallidum, anything that touches this lesion becomes a potential vehicle for spreading the infection. Any type of contact can give infection because no one can be sure that their skin is completely intact without microlesions, especially in the genital areas during sexual intercourse which is still a traumatic event. Treponema here finds more room to enter. The areas most frequently exposed to microlesions during intercourse are the glans and the preputial balano groove. When the bladder full of bacteria lyses and becomes an ulcer, all bacteria go everywhere,

Secondary phase (2-8 weeks after the 1st)
The secondary phase occurs after a few days, but sometimes even 1/2 months from the lesion, the bacterium passes through small lymphatic or venous vessels arriving at the bloodstream where it is distributed systemically throughout the body. Now we have disparate symptoms and some specific ones and they can be:
Fever and other similar flu symptoms: asthenia, difficulty in performing daily or work tasks, photophobia, lung problems, severe headaches, chills, nuchal stiffness (symptom of meningitis after flu).
Generalized systemic lymphadenopathy, as for aids, that is an enlargement of the lymph node stations of the whole body that represents the immune response of the organism to the germ, creates an inflammation. When there is inflammation in the lymph node stations the lymph nodes swell (for example, when there is a gum infection that drains into the submandibular lymph node), if they are painful to the touch this is a positive fact it means that it is a reactive inflammatory lymph node, quite different from a painless swelling that indicates a mass that is growing and that can be a metastasis.
Aseptic meningitis which, however, in the case of syphilis is spontaneously resolved, but with a certain symptomatological importance (nuchal rigidity).
Skin rash or a very characteristic rash that consists in the presence on the body of many lesions, first vesicular, then ulcerative and then necrotic, sometimes a whitish pus is formed that indicates the destruction of everything, both immunity cells and bacteria. They seem to be a lot of furuncles with the pus. The peculiar thing is that the pus usually forms when these lesions open presenting as whitish flakes, in these conditions the syphilis is recognizable with certainty and from this moment on everything that touches is highly infectious see Figure 4. Today we know the risks and danger of this bacterium and everything around the patient, even in the place where he lives must be sterilized by boiling.

Consequences of the untreated secondary form
Considering the consequences of this secondary form where you usually see the patient for the first time. Primary syphiloma is painful in the inoculum site, then it becomes painful in the groin and inguinal lymph nodes that are activated by draining the lymph. In both women and men, if it is not the primary syphiloma that causes problems of pain, it is the lymph nodes and groin that alarm the patient. Sometimes, however, the patient waits for it to heal passively and reach the next stage. Every liquid in the patient's body is highly infected in both the primary and secondary phases. If syphilis is not recognized and therefore not treated with antibiotics, the disease progresses naturally from the secondary phase in three possible ways:
- Spontaneous resolution**: 1/3 of infected patients undergo spontaneous healing with eradication of the disease, the germ is no longer present in the body, it can no longer be transmitted.
- Infected without symptoms**: 1/3 of infected patients remain infected with a sort of compromise with the immune system that has not been strong enough to carry out an eradication, the bacterium replicates again while each time the body tries to fight them. A sort of coexistence of the germ with the body is established, making the body a sort of healthy carrier who has no symptoms because their immunity preserves them from progression into the tertiary phase, but these patients continue to produce bacteria and this makes them diffusers all over the world.
- Tertiary syphilis**: 1/3 of infected patients go to the final tertiary phase, it is no longer the bacterial disease that leads to death, but the attempt of our immune system to eradicate in every possible way the bacterium with a force and a disorganization so global that in the end these immune forces turn the attack on the cellular antigens of the person. This leads to an autoimmune disease that leads to death. Syphilis leads to death because motor neurons are affected causing permanent paralysis.
Tertiary phase (years after infection)
The tertiary phase begins after many years since the patient believes to be cured (latency phase) the symptoms are very serious. Cardiovascular symptoms that sometimes even compromise the cardiovascular system and cause instant death usually after aneurysms of the aortic arch. The expression 'syphilitic aortite' indicates the moment before the aneurysm, which consists of inflammation and weakening of the aortic arch.
What you see most frequently is the consumption of organ and skin, patients 'lose pieces' as happens in leprosy, cavities that form in the skin, subcutaneous, dermis, painless because of the immune system that affects the body itself. These areas are called gums, painless because they have no inflammation so much so that the patient does not even notice it and are the site where the madness of the immune system has managed to win the fight after a phase of latency, the bacterium is no longer there, but the damage it does is more serious than the balance in the case of a healthy carrier.
The neurosyphilis is the moment in which the disease goes to various parts of innervation in various organs, it affects the motor neurons damaging them in such a way as to make them no longer functional. When the motor neuron no longer gives impulse to the muscle, it paralyses, leading to total paresis or dorsal tabe. The initial phase of total paralysis at the level of the spinal ganglia, then of the lower limbs, upper limbs and the whole body, lastly the involuntary muscles such as heart or diaphragm. Death is caused either by a blockage of the heart or the diaphragm.
Diagnosis
Primary and secondary phases, if recognized, can be fully resolved within a few weeks.
The latency phase, on the other hand, does not show symptoms because there is a balance between the immune system active against the bacterium and the proliferation of the bacterium itself. Nothing can be done in the tertiary phase because the germ is no longer present and the patient's condition becomes a pure, very aggressive autoimmune disease.
Primary Diagnosis: Microscopy in the dark field or you isolated the bacterium in the rabbit testis in the past
Today: antibodies against Treponema Pallidum Pallidum, typical of syphilis, are sought which appear from about 7-10 days after the beginning of the lesion.
Serological diagnosis: this is the only one that can be done today because it avoids contact with bacteria. There are two types of tests:
Non-treponemic, non-primary tests that do not use the bacterium to assess the ability of antibodies to recognize it;
Treponemic tests, use the bacterium as a target for blood antibodies.
VDRL test - Venereal Disease Research Laboratory
Indirect, not treponemic, test that explains the ability of our organism to destroy itself during autoimmunity. It is a flocculation test in which antibodies produced against Treponema Pallidum during the primary and secondary phase target cardiolipin. This is a very small lipopeptide that is present in all the cells of our body, was initially extracted from the muscle of the myocardium, and if inoculated into our body is aptene, ie not by antibodies, but is specifically recognized by anti-treponema antibodies. This is because Treponema has lipidic antigens that resemble cardiolipin.
A crazy immune system does not realize that producing antibodies against the bacterium is also attacking self molecules, so to kill the bacterium tags the cardiolipin and other cross-reactive mimetic molecules of the body itself and this causes an autoimmune disease.
During the flocculation test, I put a lipid on a well in a certain amount, as all lipids float, I put in this liquid the patient's serum to see if there are antibodies against Treponema that in case there are recognize the cardiolipin. If nothing happens there are no antibodies in the serum, if a flocculation occurs the antibodies are there. Flocculation is the thickening of antibodies and cardiolipins that form a network of molecules that groups together in a single block all the recognized cardiolipins until they become a mass visible to the naked eye as a white flake. The molecule itself would not be visible but what affects the recognition and blocking of many of these molecules to form various white flakes here and there on the slide. The test can be performed in any temperature and environment in the world without any particular instrumentation. The only precaution is to make the blood sample in an aseptic manner.
Positive test = there are antibodies = confirmation must follow
Negative test = there are no antibodies = no cross-activity = patient not affected
In case of positive VDRL test (being indirect, surrogate, and not very specific) the treponemic test follows for confirmation. In fact, it must be excluded that the patient has another type of autoimmune disease that, although it has nothing to do with syphilis, produces antibodies against cardiolipin, in this case I can not say that the patient is syphilitic.
Treponemic tests
The treponemic test, instead, uses treponemic antigens of Treponema Pallidum Pallidum.
In the case of the fluorescence reaction we will see only the bacterium placed on the slide in immunofluorescence and we see the ability of the antibodies of the patient's serum to recognize this bacterium. With fluorescent antisera, human antimmunoglobulins, these second antibodies are placed after the first (serum), which recognize the human Ig to the bacterium and this becomes completely fluorescent green. However, this suggests that the industry should grow the Treponemi Pallidum Pallidum in the testicles of rabbits, purify them, put them on the slide, fix them and send them to the laboratory for immunofluorescence. All this entails problems such as: the technicians who work in these industries exposed to risks, costs, the sacrifice of animals.
It is an indirect immunofluorescence test because it is not the first antibody (that of the patient's serum) that is marked and fluorescent, but it is the second antibody, that binds the human immunoglobulins, produced in sheep or horses immunized with human antibodies. They are universal antisera that recognize all human Ig and are conjugated with a fluorochrome (usually fluorescein). After several washes the bacteria appear green because they are surrounded by antibodies that are recognized by the second labeled antibodies, hence the fact that this diagnosis is indirect.
If it were a direct immunofluorescence, the monoclonal antibody binding the treponema antigen would be fluorescent.
Today genetic engineering has opened up new possibilities; recombinant Treponema antigens can be produced in bacteria, for example the Treponema antigen can be expressed by Escherichia Coli. Once the antigen was extracted with complex methods, I obtained typical and specific antigens of Treponema Pallidum that no other microorganism has in its structure. These antigens are proteins that can be subjected to various tests. It is necessary to find a type of test that can be carried out anywhere and without special equipment, such as the TPHA.
TPHA (Treponema Pallidum Haemagglutination Assay)
Universal and easy haemagglutination test with antibodies that see red blood cells, bind them and form a network. In the healthy organism this does not happen, there are no antibodies against the red blood cells of animals of another species because having never made contact with these blood cells does not develop any immune reaction, unless there is a viral disease that leads to their development that we will see later, in general we can say that these antibodies are not there. Assuming this, if you put the blood cells in a small well with a 'U' bottom, after a certain amount of time thanks to the force of gravity they settle on the bottom and I see a small red circle, you add the patient's serum and you do not observe any change.
To effectively diagnose this disease, the test described above must be performed after adding particular molecules to the surface of the red blood cells. Treponema antigens that are not infectious are attached to the blood cell, purified and glued. For the attack it is sufficient to put the globules in tannic acid that makes their surface sticky, add the antigens and shake for maximum effectiveness of the practice. Afterwards, it is left to settle or alternatively centrifuged, the acid is replaced by a saline solution. They return normal and shiny with Treponema antigens on their surface, now the globules are vehicles of new substances recognized by antibodies that have formed against Treponema Pallidum. Alongside normal red blood cells are red blood cells with antigens and by placing the serum I can distinguish two different situations:
Negative serum, does not recognize anything and as described in the general situation the red blood cells go to the bottom.
Positive serum, has inside antibodies against Treponema Pallidum that bind creating a mesh, three-dimensional network, in which I understand that the serum is positive. This mesh, in which the globules are held together by the antibodies against the antigen they have on the surface, is large and goes down like the individual globules, it is possible to distinguish from the previous case because the red dot is no longer visible. If I dilute the serum several times the dot will be visible again, if for example this happens after diluting a thousand times then the maximum antibody titer of that serum is 1/1000. This is because there are not enough antibodies to form a mesh and the globules settle at the bottom as in the previous case.
These samples can be stored at room temperature so the test can be performed anywhere. Tertiary syphilis with this method is difficult to diagnose because the antibodies are cross-reactive against almost everything.
At this point the VRDL test is repeated
Negative VDRL: non-infected patient
VDRL positive: infected or false positive patient to be tested with a specific treponemic test better than fluorescence TPHA. If it is confirmed with the flocculation test it is therefore the patient is affected.
VDRL is also important after treatment because to ensure that the patient is cured the VDRL must be negative. With healing, the previously visible non-specific part of the antibodies disappears, while the B lymphocytes, which produce the ever-present memory antibodies, produce more specific antibodies to the treponema antigens. It is not possible to make an evaluation of healing by a TPHA test on the basis of the disappearance of antibodies because the antigens on the red blood cells are specific and will be recognized by my immune memory.
While if the patient is healed and therefore the antibiotics have taken effect, the reactivity against cardiolipin disappears, so a few weeks or days from the start of treatment the VDRL becomes negative and when this happens it means that the patient is healing.
Treatment
The patient is given beta-lactam. Each beta-lactam is active against Treponema: both penicillins and cephalosporins. Obviously, when you get to a tertiary syphilis it is useless to take antibiotics because there is no longer the bacterium. The dose of the antibiotic depends on the phase. In some cases there is a reaction called Jarisch-Herxheimer, in which the beta-lactam creates a lysis of the Treponemas in the blood releasing an endotoxin, being the bacterium of the type gram negative, you should not imagine, however, large amounts of this toxin. The symptoms are chills, fever, general malaise. In this case, a negative VDRL is expected.
Depending on the severity of the symptoms and therefore the stage of the disease, the dose varies from normal to massive.
Curiosity and evolution of therapy over time
Syphilis came from America and spread to France during the Napoleonic era so much so that it was called 'bad French', a funny fact is that the French in turn called syphilis 'bad Neapolitan' passing the responsibility on to the Italians.
Previously it was treated with the administration of mercury salts and arsenic salts. Obviously these substances were very toxic, but if the patient did not die after about six months of treatment, it was the micro-organism that bore the burden of living in an intoxicated host.
It was cured by the death of bacteria that did not resist the toxicity that had been created in the environment in which they lived. To this day, this therapy has not been abandoned and arsenic salts are used in conjunction with beta-lactams to achieve a much faster recovery. Between the end of the 18th century and the beginning of the 19th century the medicine was empirical, today the dose is calculated much more precisely.
Spirochete
Le spirochete sono molto importanti dal punto di vista medico e patologico perché causano malattie di una certa gravità, molte volte anche mortali.
Una di queste, tristemente nota, causata da una specie chiamata Treponema Pallidum Pallidum, è la sifilide.
Caratteristiche generali delle spirochete
• Batteri Gram negativi
• Molto mobili per la presenza di flagelli all'interno della membrana esterna, per questo detti endoflagelli che li fanno muovere quasi come fossero dei serpenti. Questi organelli forniscono loro una forma a spirale o mollettina e da qui il nome di spirochete.
• Dimensioni: notevole lunghezza ma spessore ridotto (< 0,5 micrometri), forma a bacillo o meglio spirillo.
• Non facilmente visibili con il microscopio ottico, perciò viene utilizzato un microscopio in campo oscuro, e non possono essere individuati con una colorazione di Gram, ma sono necessari delle colorazioni più complesse.
.
• Diagnosticare questi batteri è abbastanza complesso sia per quanto riguarda l'isolamento, la colorazione e anche la diagnosi indiretta della loro presenza attraverso la formazione di anticorpi.
• Normalmente sono patogene e causano mattie gravi nell'uomo, in molti casi, invece, le spirochete sono commensali di tanti organismi. Per esempio: spirochete nel cavo orale dell’uomo che compartecipano a formare quel biofilm microbico che è la base sui cui si costituisce la flora batterica commensale.
Gran parte di questi batteri attraverso lo spazzolare dei denti arrivano occasionalmente nel sangue dando delle reazioni immunitarie sebbene facciano parte della flora dell'organismo stesso, e queste reazioni fanno interferenza quando si pratica una diagnosi sierologica di queste malattie, in particolare della sifilide.
Sono tre principalmente i generi che appartengono alla famiglia delle spirochetacee:
• Borrelia = capaci di dare infezioni anche gravi e malattie autoimmunitarie;
• Leptospira = Frequente nelle aree padane per l'alta presenza di roditori, può essere mortale;
• Treponema = è il genere che comporta più problematiche e che produce il ceppo della sifilide, oggi in netto aumento nei nostri Paesi, è quindi importante prenderne in considerazione la gravità.
La sifilide
• La malattia è estesa in tutto il mondo ed è grave.
• Batterio che causa questa malattia è il Treponema Pallidum della sottospecie Pallidum (nome completo nella catalogazione è Treponema Pallidum Pallidum), è una classica spirocheta con forma a spirillo o mollettina, è un Gram negativo e l'uomo è l'unico ospite riconosciuto (non è una zoonosi che si può contrarre da altri animali, si trasmette solo da uomo a uomo).
Isolamento
Fino a poco tempo fa era coltivato in animali particolarmente suscettibili come i conigli, in particolare nei testicoli. Una volta inoculato in questo distretto il batterio riesce a crescere in quantità notevoli dando ingrossamento del sacco testicolare, il liquido biologico prelevato dal testicolo da origine a miliardi e miliardi di batteri vivi e pericolosi. Quindi questo è l'unico modo per isolarli.
Oggi non si pratica più per motivi legati alla salute dei conigli e anche a quella dell'uomo, infatti con il metodo appena illustrato erano alte le probabilità di infezione a danno dei tecnici di laboratorio. Questa malattia si contrae anche solo per contatto, se le aree della cute esposte al batterio hanno lesioni, perchè il batterio essendo sottilissimo è in grado di passare anche attraverso piccolissime ferite della cute e dare infezione da sifilide. A causa di questa sua sottigliezza, pur essendo un Gram negativo, non si colora con la colorazione tipica di questa classe di batteri
Si vede vivo e se ne apprezzano i movimenti con il microscopio in campo oscuro. Non è quello classico con il vetrino, ma c'è un piccolo avvallamento di vetro nero nel porta-oggetti in cui viene depositata una goccia del campione.
Il concetto su cui si basa questo microscopio è simile a quello del cielo di notte, noi siamo nella parte scura della Terra, il Sole sta dietro di noi e la Luna riflette la luce del Sole, non la propria, rendendosi visibile dalla Terra. La riflessione della luce policromatica ci appare bianca, essendo l'insieme degli spettri.
Questa stessa luce è quella che vediamo con i batteri se messi della celletta e illuminati, non da sotto, ma dal lato, il vetro lascia passare la luce e quello che ritorna a noi è la luce riflessa dei batteri. Insieme alla luce riflessa si può vedere la motilità di questi microrganismi che sono a spirale e come dei serpenti si muovono velocissimi nel liquido
Test di neutralizzazione di Nelson
In passato questa motilità è stata sfruttata per un test di neutralizzazione, chiamato test di Nelson che era volto a vedere se nel corpo umano ci fossero anticorpi capaci di bloccare questi batteri e quindi di neutralizzarne l'attività patogenetica. La procedura prevedeva l’uso del microscopio in campo oscuro e l’aggiunta di una goccia di siero del paziente sul batterio Treponema Pallidum.
Se si osservava la formazione di ammassi agglutinati non più funzionali questi indicavano che il paziente aveva sviluppato anticorpi neutralizzanti e che quindi poteva andare incontro a guarigione spontanea della malattia. Oggi il campo oscuro è stato abolito sia per la visualizzazione del batterio che per lo svolgimento del test di Nelson, a causa dell’alta pericolosità. Tanti tecnici si sono infettati di sifilide soltanto manipolando campioni biologici o lavorando con materiale vitale.
Soggetti maggiormente esposti alla malattia
Principalmente è una malattia che si trasmette sessualmente, la sifilide oggi è in grande espansione anche in Europa dove aveva avuto un blocco tra gli anni 60-70, sta di nuovo esplodendo tra i giovani perché si contrae comunemente con un rapporto sessuale. I più colpiti:
• I 'sex workers', i lavoratori del sesso, gli omosessuali
• In generale chiunque abbia un rapporto sessuale è a rischio (endemic among sex practicers)
• chi fa uso di farmaci e droghe illegali
• Si può trasmettere anche attraverso un semplice bacio senza sesso, questa pratica è detta petting.
• Chi si sottopone a trasfusione di sangue, ma con le procedure e i controlli che vengono effettuati oggi in Paesi sviluppati non dovrebbe accadere nulla.
• Chi è a contatto con il batterio, ad esempio con l'accidentale inoculazione diretta del batterio del sangue nei laboratori
.
• Si può affermare che qualunque cosa si faccia che preveda scambio di sangue, saliva, liquidi biologici, manipolazione del batterio con frequenza può causare l'infezione. Il batterio passa anche dalla madre al il feto durante la gestazione o al neonato durante un parto naturale. Spesso l'infezione in utero porta alla morte del feto. La nascita di un neonato infettato nell'utero o all'atto della nascita comporta a ritardo mentale importante e diverse malformazioni. In queste condizioni solo non conoscendo la storia della gestante si procederebbe a un parto naturale, che risulta rischioso, altrimenti si effettuerebbe un cesareo. Nell'ambito dell'embriogenesi fino allo sviluppo del feto vede questo essere suscettibile a un'infezione gravissima da Treponema Pallidum Pallidum.
Stadi della malattia
La sifilide ha diversi stadi, il cui ultimo è mortale, ma è nel primo e nel secondo che si presentano tanti batteri nel corpo infetto e che quindi risulta infettante per le persone che lo circondano. Oggi si ritiene che anche il sudore di queste persone sia infettante, quindi tutto ciò che toccano e gli indumenti risultano essere possibili veicoli della malattia.
Sia nella fase primaria che secondaria il paziente è altamente infettante, in queste fasi le lesioni attive possono essere sulle labbra, nel cavo orale, sui genitali, o nelle zone che sessualmente parlando possono essere di facile scambio di materiale infetto. Una volta che, durante la fase secondaria, il batterio entra nel sangue è capace di andare in tutto il corpo e arrivare fino al sistema nervoso centrale creando un'infezione multiorgano che si manifesta con sintomi eclatanti non facilmente confondibili con altre patologie.
È una malattia cronica, lentamente progressiva, e che non si manifesta chiaramente subito, la fase terziaria arriva solo dopo 10-20 anni come l'AIDS, durante questo periodo di latenza il paziente è comunque infettante. Mentre il secondo stadio arriva subito dopo il primo e quindi la malattia è veloce, dopo il secondo stadio c'è un periodo di latenza che può essere più o meno lungo ed è il momento in cui si capisce se il paziente è riuscito a guarire, se è riuscito a controllare la malattia, ma non a eradicarla diventando, quindi, un portatore sano oppure se va in contro alla fase terziaria, finale e mortale. Ogni fase presenta dei fenomeni e dei sintomi unici e dal punto di vista pratico risulta inconfondibile.
1. Fase primaria (6 gg-1 mese)
La prima fase detta anche “cancroide” inizia con una vescicola piena di liquido che si manifesta nel punto di inoculo del batterio, ossia dove ha trovato la lesione ed è entrato nella mucosa, nel derma comincia a proliferare. La replicazione dà origine a una forma di vescicola che può evolvere in un'ulcera piena di Treponema Pallidum, qualsiasi cosa tocchi questa lesione diventa un potenziale veicolo di diffusione dell'infezione . Qualsiasi tipo di contatto può dare infezione perché nessuno può essere sicuro di avere la pelle completamente integra senza microlesioni, specialmente nelle zone genitali durante un rapporto sessuale che è comunque un evento traumatico. Il Treponema qui trova più spazio per entrare. Le zone più frequentemente esposte a microlesioni durante un rapporto sono il glande e il solco balano prepuziale. Quando la vescicola piena di batteri si lisa diventando ulcera tutti i batteri vanno ovunque,
2. Fase secondaria (2-8 settimane dopo la 1°)
La fase secondaria si presenta dopo pochi giorni, ma a volte anche 1/2 mesi dalla lesione, il batterio attraversa piccoli vasi linfatici o venosi arrivando al circolo sanguigno dove si distribuisce in via sistemica in tutto l'organismo. Ora si hanno sintomi disparati e alcuni specifici e possono essere:
• Febbre e altri sintomi simili influenzali: astenia, difficoltà nello svolgere i compiti giornalieri o lavorativi, fotofobia, problemi polmonari, forti cefalee, brividi, rigidità nucale (sintomo di meningite dopo influenza).
• Linfadenopatia sistemica generalizzata, come per l'aids, ovvero un ingrossamento delle stazioni linfonodali di tutto il corpo che rappresenta la risposta immunitaria dell'organismo al germe, si crea un’infiammazione. Quando c'è infiammazione nelle stazioni linfonodali i linfonodi si ingrossano (ad esempio quando si ha un'infezione gengivale che drena nel linfonodo sottomandibolare), se al tatto risultano dolenti questo è un fatto positivo significa che è un linfonodo infiammatorio reattivo, ben diversa da un ingrossamento senza dolore che indica una massa che sta crescendo e che può essere una metastasi.
• Meningite asettica che però nel caso della sifilide è a risoluzione spontanea, ma comunque con una certa importanza sintomatologica (rigidità nucale).
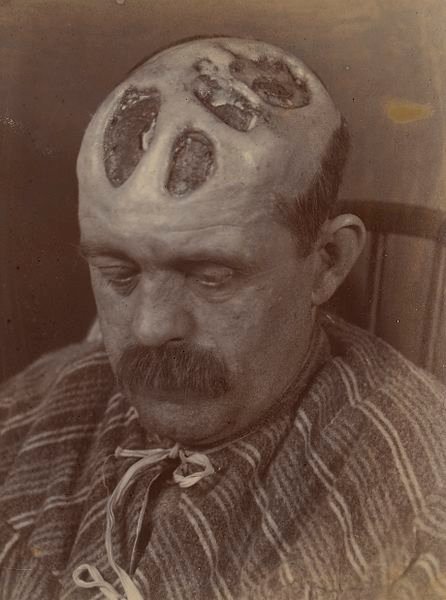
• Rash cutaneo o esantema molto caratteristico che consiste nella presenza sul corpo di molte lesioni prima vescicolari, poi ulcerose e in seguito necrotiche, talvolta si forma un pus biancastro che indica la distruzione di tutto sia cellule dell'immunità che dei batteri. Sembrano tantissimi foruncoli con il pus. La cosa peculiare è che il pus di solito si forma quando queste lesioni si aprono presentandosi come dei fiocchi biancastri, in queste condizioni la sifilide è riconoscibile con certezza e da questo momento in poi tutto quello che tocca è altamente infettante vedi Figura 4. Oggi si conoscono i rischi e la pericolosità di questo batterio e tutto ciò che circonda il paziente, anche nel luogo in cui vive deve essere sterilizzato per bollitura.
Conseguenze della forma secondaria non trattata
Considerando le conseguenze di questa forma secondaria dove solitamente si vede per la prima volta il paziente. Il sifiloma primario è dolente nella sede di inoculo, poi lo diventa anche a livello dell'inguine e dei linfonodi inguinali che si attivano drenando la linfa. Sia nella donna che nell'uomo se non è il sifiloma primario a dare problemi di dolorabilità sono i linfonodi e l'inguine ad allarmare il paziente. A volte nonostante ciò, il paziente aspetta che questo guarisca passivamente giungendo alla fase successiva. Ogni liquido del corpo del paziente è altamente infetto sia nella fase primaria che secondaria. Se la sifilide non viene riconosciuta e quindi non viene trattata con antibiotici la malattia progredisce in modo naturale dalla fase secondaria seguendo tre possibili vie:
• Risoluzione spontanea: 1/3 dei pazienti infetti vanno incontro a guarigione spontanea con eradicazione della malattia, il germe non è più presente nel corpo, non si può più trasmettere.
• Infetti senza sintomi: 1/3 dei pazienti infetti rimangono tali con una sorta di compromesso con il sistema immunitario che non è stato abbastanza forte per effettuare un'eradicazione, il batterio replica ancora mentre ogni volta il corpo cerca di combatterli. Si instaura una specie di convivenza del germe con il corpo facendo dell'organismo una sorta di portatore sano che non ha sintomi perché la loro immunità li preserva dalla progressione in fase terziaria, ma questi pazienti continuano comunque a produrre batteri e questo fa di loro dei diffusori in tutto il mondo .
• Sifilide terziaria: 1/3 dei pazienti infetti va incontro alla fase terziaria finale, non è più la malattia batterica che porta a morte, ma il tentativo del nostro sistema immunitario di debellare in tutti i modi possibili il batterio con una forza e una disorganizzazione così globali che alla fine queste forze immunitarie rivolgono l'attacco verso gli gli antigeni cellulari della persona. Si giunge a una malattia autoimmunitaria che conduce a morte. La sifilide porta a morte perché vengono colpiti i motoneuroni causando paralisi permanente.
3. Fase terziaria (anni dopo il contagio)
La fase terziaria esordisce dopo tanti anni da quando il paziente crede di essere guarito (fase di latenza) i sintomi sono molto gravi. Sintomi cardiovascolari che a volte addirittura compromettono il sistema cardiocircolatorio e causano morte istantanea solitamente dopo aneurismi dell'arco aortico. Con l'espressione 'aortite sifilitica' si indica il momento precedente all'aneurisma che consiste nell'infiammazione e nell'indebolimento dell'arco aortico.
Ciò che si vede più frequentemente è il consumo di organo e cute, i pazienti 'perde pezzi' come avviene nella lebbra, cavità che si formano nella cute, sottocute, derma, indolori a causa del sistema immunitario che colpisce l'organismo stesso. Queste aree sono chiamate gomme, indolori perché prive di infiammazione tanto è che il paziente nemmeno se ne accorge e sono il sito in cui la follia del sistema immunitario è riuscita a vincere la lotta dopo una fase di latenza, il batterio non c'è più, ma il danno che fa è più grave rispetto all'equilibrio nel caso di portatore sano.
La neurosifilide è il momento in cui la malattia va in varie parti di innervazione in vari organi, colpisce i motoneuroni danneggiandoli in maniera tale da renderli non più funzionali. Quando il motoneurone non da più impulso al muscolo questo si paralizza portando alla paresi totale o tabe dorsale. La fase iniziale della paralisi totale a livello dei gangli spinali, poi degli arti inferiori, superiori e di tutto il corpo, per ultimi i muscoli involontari quali cuore o diaframma. La morte è causata o da un blocco del cuore o del diaframma.
Diagnosi
Fasi primaria e secondaria se riconosciute possono essere totalmente risolte nel giro di poche settimane.
La fase di latenza invece non manifesta sintomi perché c'è equilibrio tra sistema immunitario attivo contro il batterio e la proliferazione del batterio stesso. Nella fase terziaria non si può fare nulla perché il germe non c'è più e la condizione del paziente diventa una pura malattia autoimmunitaria molto aggressiva.
Diagnosi Primaria: Microscopia in campo oscuro o si isolava il batterio in testicolo di coniglio nel passato
Oggi: si cercano anticorpi contro il Treponema Pallidum Pallidum tipici della sifilide che compaiono da circa 7-10 gg dopo l'inizio della lesione .
Diagnosi sierologica: è l'unica effettuabile oggi perché evita il contatto con batterio. Ci sono due tipi di test:
• Test non treponemici, non primari, che non fanno uso del batterio per valutare la capacità degli anticorpi di riconoscerlo;
• Test treponemici, fanno uso del batterio come bersaglio degli anticorpi del sangue.
Test VDRL - Venereal Disease Research Laboratory
Test indiretto, non treponemico, che spiega la capacità del nostro organismo di distruggere sé stesso durante l'autoimmunità. È un test di flocculazione in cui gli anticorpi prodotti contro il Treponema Pallidum durante la fase primaria e secondaria riconoscono come bersaglio la cardiolipina. Questa è un piccolissimo lipopeptide che è presente in tutte le cellule del nostro corpo, inizialmente è stato estratto dal muscolo del miocardio, e se inoculato nel nostro corpo è aptene, ossia non da anticorpi, ma è riconosciuto specificamente da anticorpi anti-treponema. Questo avviene perché il Treponema ha antigeni lipidici che somigliano alla cardiolipina.
Un sistema immunitario impazzito non si accorge che producendo anticorpi contro il batterio sta attaccando anche molecole self, perciò per uccidere il batterio targhetta la cardiolipina e altre molecole cross reattive mimetiche dell'organismo stesso e ciò causa una malattia autoimmunitaria
Durante il test di flocculazione, si mette un lipide su un pozzettino in una certa quantità, come tutti i lipidi galleggiano, inserisco in questo liquido il siero del paziente per vedere se ci sono anticorpi contro il Treponema che nel caso in cui ci siano riconoscono la cardiolipina. Se non succede nulla non ci sono anticorpi nel siero, se avviene una flocculazione gli anticorpi ci sono. La flocculazione è l'addensamento di anticorpi e cardiolipine che formano un reticolo di molecole che raggruppa in un unico blocco tutte le cardiolipine riconosciute fino a farle diventare una massa visualizzabile ad occhio nudo come un fiocco bianco. La molecola in sé non sarebbe visibile ma ciò che incide sul riconoscimento e il blocco di tantissime di queste molecole a formare vari fiocchi bianchi qua e là sul vetrino. Il test è eseguibile in qualsiasi temperatura e ambiente del mondo senza particolare strumentazione. L'unica accortezza è fare il prelievo di sangue in maniera asettica.
Test positivo = ci sono anticorpi = deve seguire una conferma
Test negativo = non ci sono anticorpi = nessuna cross-attività = paziente non affetto
In caso di test VDRL positivo (essendo indiretto, surrogato, e poco specifico) segue il test treponemico per conferma. Infatti, si deve escludere che paziente abbia un altro tipo di malattia autoimmunitaria che, pur non avendo niente a che vedere con la sifilide, produce anticorpi contro la cardiolipina, in questo caso non posso affermare che il paziente sia sifilitico.
Test treponemici
Il test treponemico, invece fa uso di antigeni treponemici del Treponema Pallidum Pallidum.
Nel caso della reazione di fluorescenza che vedremo si vede solo il batterio messo sul vetrino in immunofluorescenza e si nota la capacità degli anticorpi del siero del paziente di riconoscere questo batterio. Con antisieri fluorescenti, antimmunoglobuline umane, si mettono questi secondi anticorpi dopo il primo (quello del siero), che riconoscono le Ig umane al batterio e questo diventa completamente verde fluorescente. Questo però suggerisce che l'industria deve crescere i Treponemi Pallidum Pallidum nei testicoli dei conigli, purificarli, metterli sul vetrino, fissarli inviarli in laboratorio per l'immunofluorescenza. Tutto ciò comporta problemi quali: i tecnici che lavorano in queste industrie esposti ai rischi, i costi, il sacrificio di animali.
È un Test di immunofluorescenza indiretta perché non è il primo anticorpo (quello del siero del paziente) che è marcato e presenta fluorescenza, ma è il secondo anticorpo, quello che lega le immunoglobuline umane, prodotte nei montoni o nei cavalli immunizzati con anticorpi umani. Sono antisieri universali che riconoscono tutte le Ig umane e sono coniugati con un fluorocromo (solitamente la fluoresceina). Dopo vari lavaggi i batteri appaiono verdi perché circondati da anticorpi che a loro volta sono riconosciuti dai secondi anticorpi marcati, da qui il fatto che questa diagnosi sia indiretta.
Se fosse un’immunofluorescenza diretta l’anticorpo monoclonale che lega l’antigene del treponema sarebbe fluorescente.
Oggi l'ingegneria genetica ha aperto nuove possibilità, si possono produrre antigeni ricombinanti del Treponema in batteri, per esempio l'antigene del Treponema si può fare esprimere all'Escherichia Coli. Una volta estratti l'antigene con metodiche complesse ho ottenuto antigeni tipici e specifici del Treponema Pallidum che nessun altro microorganismo ha nella sua struttura. Questi antigeni sono proteine che possono essere sottoposte a vari test. È necessario trovare un tipo di test che può essere svolto ovunque e senza particolari strumentazioni, esempio il TPHA.
TPHA (Treponema Pallidum Haemagglutination Assay)
Test di emoagglutinazione, universale e facile con anticorpi che vedono i globuli rossi, li legano e formano un reticolo. Nell'organismo sano questo non succede, non ci sono anticorpi contro i globuli rossi di animali di un'altra specie perché non avendo mai preso contatto con questi globuli non si sviluppa nessuna reazione immunitaria, tranne nel caso in cui ci sia una malattia virale che porta al loro sviluppo che si vedrà in seguito, in generale possiamo affermare che questi anticorpi non ci sono. Dando per scontato questo, se si mettono i globuli in un pozzettino con un fondo a 'U', dopo un certo lasso di tempo grazie alla forza di gravità sedimentano sul fondo e vedo un piccolo cerchio rosso, si aggiunge il siero del paziente e non si osserva alcun cambiamento.
Per diagnosticare effettivamente questa malattia occorre eseguire il test precedentemente descritto dopo aver aggiunto molecole particolari sulla superficie dei globuli rossi. Si attaccano al globulo gli antigeni del Treponema che non sono infettanti, vengono purificati e incollati. Per l'attacco è sufficiente mettere i globuli in acido tannico che rende collosa la loro superficie, aggiungere gli antigeni e agitare per la massima efficacia della pratica. In seguito, si lascia sedimentare o alternativamente si centrifuga, viene sostituito l'acido con una soluzione fisiologica. Tornano normali e lucidi con antigeni del Treponema sulla loro superficie, ora i globuli sono veicoli di nuove sostanze riconosciute da anticorpi che si sono formati contro il Treponema Pallidum. Si affiancano a globuli rossi normali i globuli rossi con antigeni e mettendo il siero posso distinguere due diverse situazioni:
• Siero negativo, non riconosce niente e come descritto nella situazione generale i globuli rossi vanno sul fondo.
• Siero positivo, presenta al suo interno anticorpi contro il Treponema Pallidum che si legano creando una maglia, rete tridimensionale, in cui capisco che il siero è positivo. Questa maglia, in cui i globuli sono tenuti insieme dagli anticorpi contro l'antigene che hanno sulla superficie, è grossa e va giù come i singoli globuli, si riesce a distinguere dal caso precedente perché non è più visibile il puntino rosso. Se diluisco il siero più volte il puntino sarà di nuovo visibile, se per esempio questo accade dopo aver diluito mille volte allora il titolo massimo anticorpale di quel siero è 1/1000. Questo accade perché non ci sono anticorpi sufficienti per formare una maglia e i globuli sedimentano sul fondo come nel caso precedente.
Questi campioni sono conservabili a temperatura ambiente quindi il test può essere effettuato dappertutto. La sifilide terziaria con questo metodo è difficile da diagnosticare perché gli anticorpi sono cross-reattivi contro quasi tutto.
A questo punto si ripete il test VRDL
• VDRL negativa: paziente non infetto
• VDRL positiva: paziente infetto o falso positivo da verificare con test treponemico specifico meglio TPHA rispetto alla fluorescenza. Se viene confermato con il test della flocculazione è quindi il paziente è affetto.
Il VDRL è importante anche dopo il trattamento perché per accertarsi che il paziente sia guarito la VDRL si deve negativizzare. Con la guarigione sparisce la parte aspecifica degli anticorpi che prima era visibile, mentre i linfociti B, che producono gli anticorpi di memoria sempre presenti, producono anticorpi più specifici verso gli antigeni del treponema. Non è possibile fare una valutazione di guarigione attraverso un test TPHA sulla base della scomparsa degli anticorpi perché gli antigeni sui globuli rossi sono specifici e saranno riconosciuti dalla mia memoria immunitaria.
Mentre se il paziente è guarito e quindi gli antibiotici hanno fatto effetto, sparisce la reattività contro la cardiolipina, quindi poche settimane o pochi giorni dall'inizio del trattamento la VDRL diventa negativa e quando questo avviene significa che il paziente sta guarendo.
Trattamento
Al paziente vengono somministrati i beta lattamici. Ogni beta-lattamico è attivo contro il Treponema: sia le penicilline che le cefalosporine. Ovviamente quando si arriva a una sifilide terziaria è inutile assumere antibiotici perché non c'è più il batterio. La dose dell'antibiotico dipende dalla fase. In alcuni casi si verifica una reazione detta Jarisch-Herxheimer, in cui il beta lattamico crea una lisi dei Treponemi nel sangue liberando un'endotossina, essendo il batterio del tipo gram negativo, non bisogna immaginarsi però grosse quantità di questa tossina. I sintomi sono brividi, febbre, malessere generale. In questo caso ci si aspetta una VDRL negativa.
In base alla gravità dei sintomi e quindi allo stadio della malattia la dose varia da normale a massiccia.
Curiosità e evoluzione nel tempo della terapia
La sifilide è arrivata dall'America e diffusasi in Francia durante l'epoca di Napoleone tanto da essere stata chiamata 'mal francese', un fatto divertente è che i francesi a loro volta chiamavano la sifilide 'mal napoletano' scaricando la responsabilià sugli italiani
Prima veniva trattata con la somministrazione di sali di mercurio e sali di arsenico. Ovviamente queste sostanze erano molte tossiche, ma se il paziente non moriva dopo sei mesi circa di cura era il microrganismo a sopperire non sopportando di vivere in un ospite intossicato.
Si guariva per la morte dei batteri che non resistevano alla tossicità che si era creata nell'ambiente in cui vivevano. Tutt'ora questa terapia non è stata abbandonata e i sali di arsenico si usano insieme ai beta lattamici per ottenere una guarigione molto più veloce. Tra la fine del '700 e gli inizi dell'800 il medicamento era empirico, oggi la dose è calcolata in modo molto più preciso.
Fonti/Sources
Immagini/Pictures
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Good post, but please add a warning symbol or something like this, in the beginning, to warn people about the pictures.
Thanks
Chapper
Hello Chapper, it's fine if the contents are in your opinion strong I'll see to add in the next posts a symbol of danger or something similar, thanks for your comment
credevo la sifilide fosse scomparsa lasciando il posto ad altre patologie veneree....interessantissimo questo post
ciao wisher! è sempre bello trovarti sotto i miei post! purtroppo no, la sifilide non è mai sparita, semplicemente se ne parla poco, ma anzi è in continuo aumento negli ultimi anni, purtroppo a causa di persone che non si curano e diffondono la patologia
This post was selected, voted and shared by the discovery-it curation team in collaboration with the C-Squared Curation Collective. You can use the #Discovery-it tag to make your posts easy to find in the eyes of the curator. We also encourage you to vote @c-squared as a witness to support this project.
Hello,
Your post has been manually curated by a @stem.curate curator.
We are dedicated to supporting great content, like yours on the STEMGeeks tribe.
Please join us on discord.
Congratulations @riccc96! You have completed the following achievement on the Steem blockchain and have been rewarded with new badge(s) :
You can view your badges on your Steem Board and compare to others on the Steem Ranking
If you no longer want to receive notifications, reply to this comment with the word
STOPThis post has been voted on by the SteemSTEM curation team and voting trail. It is elligible for support from @curie and @minnowbooster.
If you appreciate the work we are doing, then consider supporting our witness @stem.witness. Additional witness support to the curie witness would be appreciated as well.
For additional information please join us on the SteemSTEM discord and to get to know the rest of the community!
Please consider using the steemstem.io app and/or including @steemstem in the list of beneficiaries of this post. This could yield a stronger support from SteemSTEM.
Spirochetes are a bit of a headache clinically to be honest.
Luckily for us, the secondary stage & neurosyphilis (the 3rd stage) are not commonly seen anymore thanks to awareness and ATB usage. We still have to learn it, in the case we encounter it, but nowadays is rare.
Even more rare are the complications you mentioned about them like Aortic Aneurysm.
Nice information!
Let's say that we can say that nowadays, in western countries the situation is as it was described by you, but unfortunately in reality different is not so different from how it was once, I'm glad that you liked the post :)