HEPATIC CIRRHOSIS
HEPATIC CIRRHOSIS
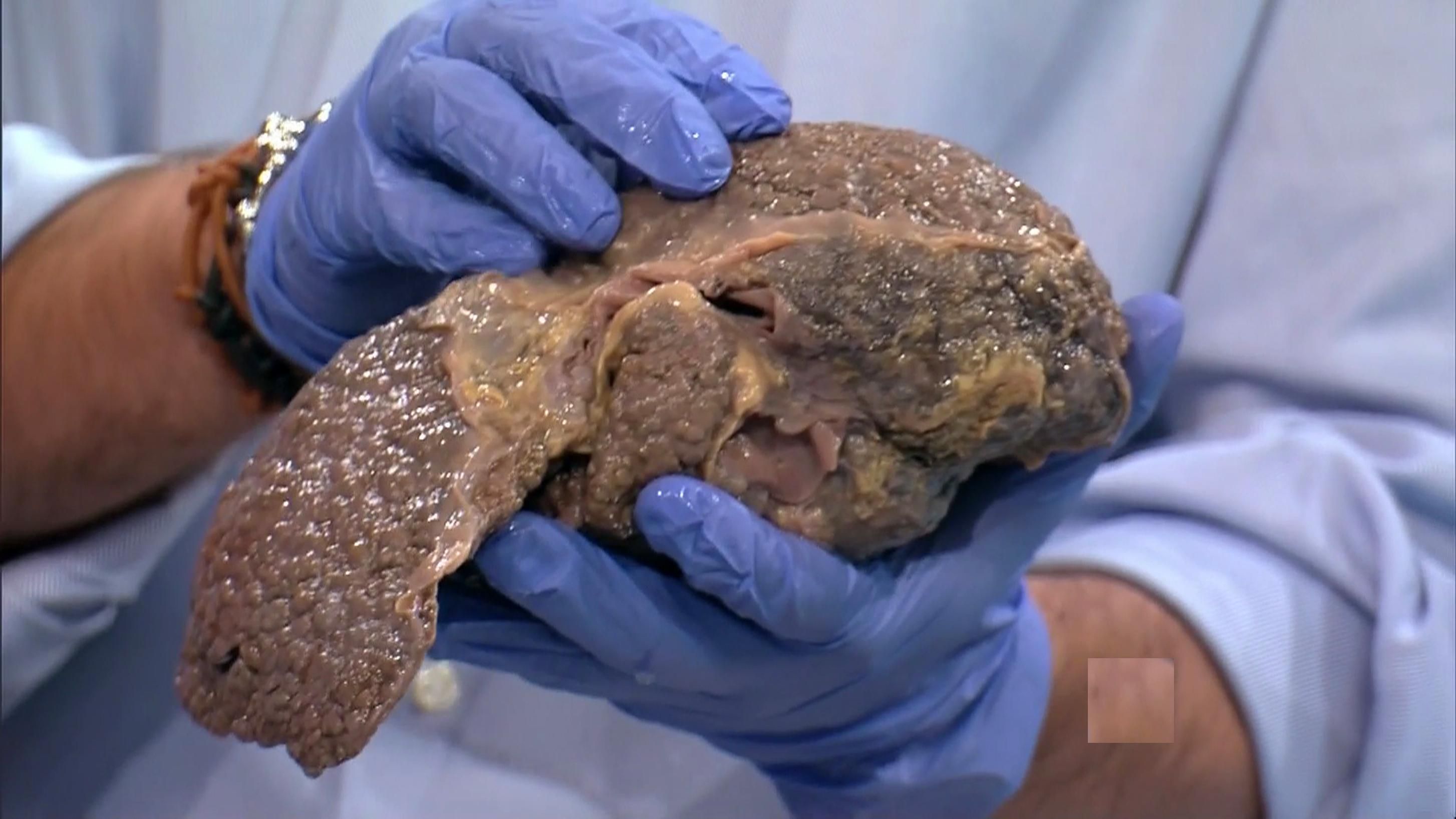
Today we talk about cirrhosis in a chronic, progressive, diffuse, irreversible and varied cause of chronic artery disease, characterized by the presence of regeneration nodules, which lead to an alteration of the vascular architecture, where the most Common: alcohol, hepatitis B and C viruses, and other agents.
Etiology
--Alcohol. Since only 20% to 25% of chronic alcoholics develop hepatic cirrhosis, it is considered that in their appearance they should play an important role as well as nutritional, immunological and genetic factors. It is suggested that alcoholic hepatitis is the precursor of cirrhosis or that there is actually a direct stimulation of fibrogenesis by alcohol.

--Hepatitis C virus: 40% of cirrhotic patients in Spain have a chronic infection with this virus, which is demonstrated by the presence of specific antibodies (defenses produced by the organism) or virus particles detected in the blood. Some of these patients were infected by receiving blood transfusions before 1991, when the virus was not known and proper blood tests were not done to check for their presence.
--The hepatitis B virus: 10% of patients with cirrhosis in Spain have a chronic infection with virus B. This percentage is higher in countries like Japan or the countries of Southeast Asia, where it is more frequent.

--Primary biliary cirrhosis. Initially the bile ducts are destroyed by an immunological reaction; Then there is inflammation, cellular necrosis with fibrosis and collagenization.
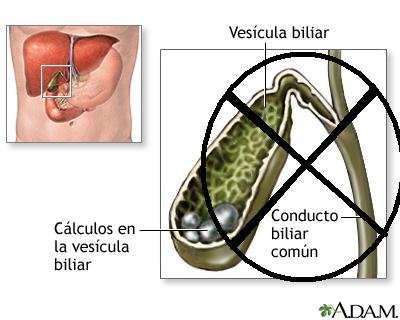
--Secondary biliary cirrhosis. It is seen in the course of conditions capable of blocking the flow for a long time (at least 3 months).
--Obstruction to venous drainage of the liver. In the final stage of any chronic venous congestion of the liver, hepatic cirrhosis (congestive heart failure, constrictive pericarditis, Budd-Chiari syndrome) may occur.
--Drugs. It is not often that the drugs produce liver cirrhosis; Has been seen with long-term methotrexate and alfametildopa, oxyphenisatin, hydralazine and amiodarone after a long period of chronic hepatitis.

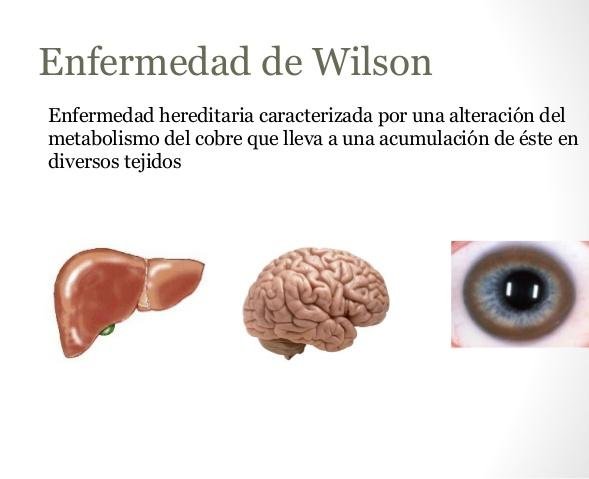
Genetic-based entities. There is a group of inherited and metabolic diseases that are accompanied by liver cirrhosis, such as hemochromatosis, alpha1-antitrypsin deficiency, Wilson's disease, galactosemia, tyrosinemia, porphyria cutanea tarda, cystic fibrosis of the pancreas and hereditary hemorrhagic telangiectasia.
Clinical picture
The onset of the disease is usually asymptomatic, which may last months or years; Other times the symptoms manifest themselves so vaguely at the beginning, that it is difficult to evaluate them. In some cases the diagnosis is accidental, and when examining the patient for other reasons hepatomegaly (enlargement of the liver) is detected with splenomegaly (enlargement of the spleen) palpable or not, as well as alterations in the liver function tests , And the diagnosis of cirrhosis is reached.
These are compensated cirrhosis; But sooner or later the disease manifests itself from the clinical point of view by one of the following syndromes: hepatic insufficiency, portal hypertension and ascites.
-*Hepatic insufficiency syndrome
Cirrhosis begins practically by any of the symptoms and signs of liver failure.
-*Asthenia. It is presented in varying degrees, depending on the evolution of the case.
.jpg)
-*Fever. The fever produced only by the activity of the hepatic affection is not frequent, reason why in front of it must be exhausted all the possibilities to demonstrate a septic process. When other causes are ruled out, the fever appears in the fourth part of the
Cirrhotic. It is moderate and maintained.

-*Pain. Often the patient manifests pain in the upper hemiabdomen, which if intensified, should make suspicion of a hepatoma.

-*Dyspepsia. Dyspnotic symptoms and flatulence are common.
-*Neuropsychiatric disorders. These symptoms range from drowsiness to coma.
Jaundice. It occurs in about half of the cases when it is not a biliary cirrhosis, in which it is constant. It is usually moderate to light, although sometimes it intensifies.
Bleeding. In decompensated cirrhosis spontaneous hemorrhages are seen anywhere in the economy, a product of the coagulation disorder that these patients present.

Edemas. They occur in approximately 50% of cases, and are usually due to hyposerinemia and water-borne disorders caused by hepatic failure.
