How big are your red blood cells? Too big? Too small? Just right? Find out here
Introduction
I am sure that most people have had blood drawn by a doctor, nurse or phlebotomist at some time or other to check it with reference to certain symptoms. Perhaps you're feeling a bit tired or listless, or even a little breathless. So what is it exactly that they are testing for and why is it a good idea for you to learn about what the test results mean?
The standard blood test is known as the complete (or full in the UK) blood count (CBC/FBC) and is performed by an automatic blood analyser. Typically, the doctor wants to see if your red blood cells (RBCs) are a little too big (macrocytosis) or a little too small (microcytosis). In both these cases, this will mean that your RBCs are unable to carry oxygen efficiently due to their not being the optimum size and shape to absorb it from the blood. This, of course, is why people with macrocytosis or microcytosis may feel a little breathless and need to sigh deeply to get enough oxygen. They may also feel tired and lethargic because they don't have enough oxygen for good aerobic respiration which is how the body produces the energy it needs to function. Less oxygen means less energy and so your body won't be able to do as much work as it needs to, e.g. create new cells, repair cellular damage or mount a robust immune response. This has potentially very serious implications as we will discuss.
For some inexplicable reason, despite having ample training and knowledge, it has come to my attention that doctors are failing to diagnose and treat what is, in my experience, a very common scenario: the presence of both macrocytosis and microcytosis with or without indications of anaemia or red flagged red cell indices. Consequently, we need to arm ourselves with sufficient knowledge to be able to interpret this test ourselves. Being able to do so could well be a matter of life and death.
For almost a decade, I have been a member of The Pernicious Anaemia Society, which helps people with both pernicious anaemia and B12 deficiency of unknown aetiology with almost 7,000 members and the Pernicious Anaemia/B12 Deficiency Support Group on Facebook which has approximately 15,000 members. There is overlap of membership, however, one thing is for certain, these people are the tiniest tip of the iceberg. The majority of them do not know what is causing their B12 deficiency and they are finding it extremely difficult to get the correct diagnosis and treatment they need from their doctors. I suspect that a very substantial proportion of these people are not being diagnosed and treated because of the problem I will describe here.
A straightforward case of anaemia
The main parameter of the CBC useful in determining macrocytosis or microcytosis is the mean corpuscular volume (MCV). The MCV is calculated by the automatic analyser by adding up the total volume of all your RBCs (haematocrit) and dividing by the total number of RBCs to get the arithmetic mean RBC volume. This is fine for the simple scenarios where a patient has either macrocytosis or microcytosis: if the MCV is above a certain value then you have enlarged RBCs and therefore a macrocytic anaemia; if it is below a certain value you have RBCs which are too small and microcytic anaemia. In the case of a macrocytic anaemia, the doctor may perform more tests to see if you have a vitamin B9 (folate) or a vitamin B12 deficiency. Similarly, in the case of iron deficiency anaemia, blood tests will be done to determine its extent.
Assuming that the doctor finds a deficiency and it is indeed the problem then you will be treated appropriately and will hopefully recover. Unfortunately, this simple, rosy scenario is frequently not quite the full story. The serum tests for folate and B12 are acknowledged to be inaccurate and difficult to interpret leading to either an overdiagnosis or underdiagnosis of these conditions: Red cell or serum folate: what to do in clinical practice?; Undetected vitamin B12 deficiency due to false normal assay results.
Note that there is another useful red cell indice called the mean corpuscular haemoglobin (MCH) which will "track" the MCV, i.e. in a pure macrocytosis the MCV and MCH will both be high and in a pure microcytosis they will both be low. This is important to appreciate for what is to follow. Essentially, both parameters mirror the size of the average RBC in these simple scenarios although that is not its intended purpose.
Also note that macrocytic RBCs contain a lot more haemoglobin than normal whereas microcytic RBCs usually contain much less. This means that MCH is less sensitive than the MCV to iron deficiency masking a macrocytosis since only macrocytic RBCs on the whole will register.
The more complex case of dimorphic anaemia
In some cases, however, you may have a combination of macrocytosis and microcytosis causing a form of anaemia known as dimorphic anaemia. Unfortunately, despite the CBC being one of the most basic tools of a doctor's trade, many do not recognise the tell-tale signs and will fail to diagnose any nutritional deficiencies at all, much less treat them. Most guidelines for doctors advise them to treat folate and B12 deficiencies when symptoms are present even if the CBC and serum tests paint an unclear picture due to the severe consequences of not doing so. Sadly, this is not happening. Someone with an undiagnosed B12 deficiency can develop permanent nerve damage and untreated it is ultimately fatal. This is why, in my opinion, everyone needs to know about this scenario and request a copy of their CBC in order to check it for themselves if necessary. That is the goal of this article and if more people are encouraged to do so we will prevent an enormous amount of chronic ill-health and unnecessary premature death.
The CBC was developed to give doctors the tools necessary to spot boundary conditions such as dimorphic anaemia because it was appreciated that the MCV alone was inadequate for the purpose. This is why: anyone who has studied basic statistics should know that when a sample has dual populations it is meaningless to calculate the arithmetic mean because there is more than one peak in the data. More sophisticated analysis techniques would be required but the automatic blood analyser simply calculates the arithmetic mean regardless. The big problem with this is that, as a result, the MCV will almost certainly be in the normal range and so the combined macrocytosis and microcytosis is effectively hidden. In order to flag up this situation, the CBC includes what are known as the red cell indices which are also known as the derived values since they are calculated from the actual measured parameters of haemoglobin, red blood cell count, etc.
An example of dimorphic anaemia
In order to keep things simple, I will just describe the case where you have a dimorphic anaemia which is predominantly a macrocytosis, i.e. they have a majority of large cells with a minority of small (the same logic can be applied to the situation where there is a minority of large cells with a majority of small cells). When the MCV is calculated it is found to be somewhere in the middle of the typical range, masking the dimorphic anaemia. However, we also have the aforementioned MCH which in the case of this patient is above the top-of-the-range. This indicates that the patient has a combined macrocytosis and microcytosis because the two parameters have diverged instead of tracking each other as in the simple case above. The patient will have deficiencies of B12, folate and iron (perhaps even copper). Unfortunately, for some reason, many doctors seem to think that since the MCV is normal, despite the red-flagged MCH, there isn't a problem. This is pure negligence since, presumably, they have received thorough training in what the CBC parameters mean at medical school given that it is one of the most basic and essential tools of their trade. They are, in effect, ignoring the straightforward science and simple statistics underpinning the meaning of the CBC.
An example of combined macrocytosis and microcytosis
In some cases, however, the problem isn't as clear cut as I have just described. Some people have deficiencies of B12, folate and iron but they are not yet severe enough to mean that their MCH or any other parameter such as MCHC are red flagged as over the top-of-the-range. It should still, however, be possible for a competent doctor to spot this situation and offer treatment given that they have only done a CBC because the patient has symptoms warranting the investigation. In this scenario, predominantly macrocytosis with a microcytosis, the MCV and MCH will be seen to diverge, i.e. the MCV will be somewhere in the middle of the range and the MCH will be towards the top of its range. This is the tell-tale sign that there is an iron deficiency reducing the size of the MCV.
The consequences of a failure to diagnose dimorphic anaemia
When you have undiagnosed and untreated vitamin and mineral deficiencies such as B12, folate and iron, this will have very severe consequences for your long term health. Many illnesses are associated with these deficiencies from heart disease to autism and ADHD, not to mention depression and many other so-called mental health issues. Failure to diagnose and treat may lead to the inappropriate prescription of various drugs which are likely to make the situation worse, not better.
Folate is essential for DNA synthesis, B12 is essential for making the myelin sheath which coats our nerves and iron is the essential component of haemoglobin. So deficiencies of these nutrients have implications for making new cells for the immune system to fight infection, keeping our nerves healthy to provide neurological functions and to carry oxygen around the body in order to produce the energy needed to keep our bodies running.
The biochemical process for which folate is essential is known as methylation. If you are folate deficient you may be experiencing hypomethylation which has been implicated in autism, ADHD and cancer.
Iron deficiency itself has also been implicated in ADHD. I suspect that that is because it is present in children who have dimorphic anaemia which is not being diagnosed.
Conclusion
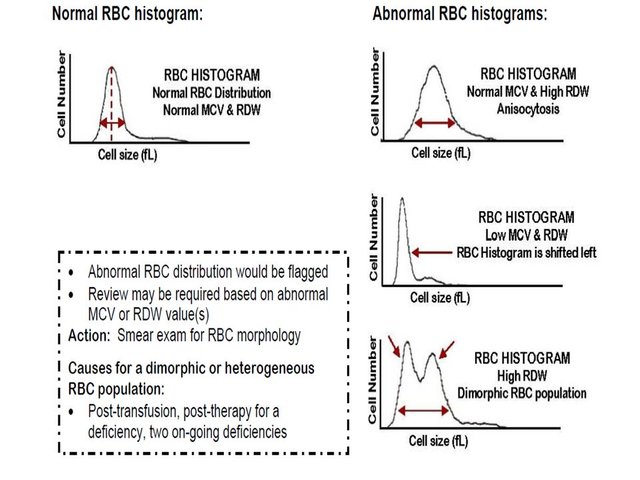
There is, in fact, a much easier way to diagnose dimorphic anaemia these days. Since around 2009, all modern blood analysers have produced graphs to go along with the numerical output of the CBC. One of these graphs is called the red cell histogram (RCH). It is, in fact, the histogram of the cellular volumes of all the RBCs, a graphical representation of the MCV. Modern blood analysers can also flag up when a sample has more than one peak as in dimorphic anaemia but the only output I've ever seen from one didn't have this flag set. With the RCH, you can tell at a glance when there is dimorphic anaemia with no need to do any serum tests at all. On the basis of the RCH a doctor should be able to flag up patients for further investigations such as peripheral blood smears or even lumber punctures. There is no excuse for any doctor to fail to diagnose and treat a patient with these simple nutritional deficiencies given the tools at their disposal.
Take a look at this paper which gives examples of what the ideal RCH should look like along with others showing dimorphic anaemia: The Red Cell Histogram and The Dimorphic Red Cell Population.
Finally, I would like the take home message of this article to be: if in doubt, always ask for a copy of your CBC from you doctor, ideally with the RCH and study it for yourself for your own piece of mind.
I will write further articles on methylation, methlyation gene polymorphisms, how to supplement them properly and strategies for recovering from the many chronic health issues caused by hypomethylation.
This diagram shows what a red cell histogram looks like from this Powerpoint presentation: http://slideplayer.com/slide/4512183/. It is actually very simple to understand.
Quite interesting article. This is the class of articles that should form the majority of submission to Steemit but usually do not get a fair reward.
Resteemed, upvoted and shared thorough discord Steemit channels in an attempt to give it more visibility.
It is important in the first days in steemit to get in touch with the community and slowly build up followers or your articles will not get visibility. I recommend you to consider joining some newbie help initiatives like minnowsupport and @steemtrail and comment other people posts.
Cheers;). I didn't know about that. I'll look into it.
Congratulations! This post has been upvoted from the communal account, @minnowsupport, by ropaga from the Minnow Support Project. It's a witness project run by aggroed, ausbitbank, teamsteem, theprophet0, and someguy123. The goal is to help Steemit grow by supporting Minnows and creating a social network. Please find us in the Peace, Abundance, and Liberty Network (PALnet) Discord Channel. It's a completely public and open space to all members of the Steemit community who voluntarily choose to be there.
If you like what we're doing please upvote this comment so we can continue to build the community account that's supporting all members.
Congratulations @jimherd! You received a personal award!
You can view your badges on your Steem Board and compare to others on the Steem Ranking
Do not miss the last post from @steemitboard:
Vote for @Steemitboard as a witness to get one more award and increased upvotes!
I tried to DM you on twitter. Seems blocked.
Posted using Partiko Android
Do we follow each other? Just @ me. My DMs aren't open.
I follow you yes. Dont know if you follow me @ same.
Posted using Partiko Android