A MUST SEE : DISEASE CAUSED BY MASTURBATION
Hey fam, so here is something I found and i find it really disturbing. I must warn you this is not for the faint hearted.

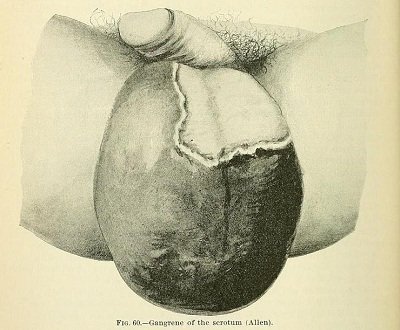
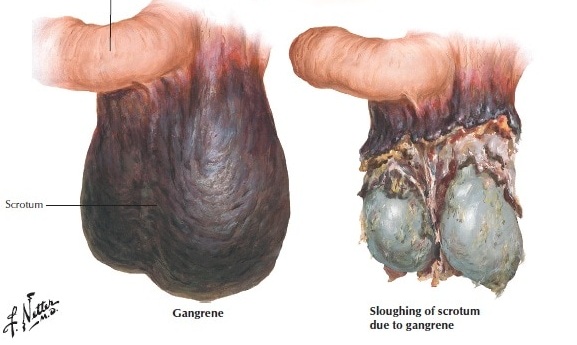
FOURNIER'S GANGRENE OF THE SCROTUM DUE TO MASTURBATION
Fournier’s gangrene is a rare and often fulminant necrotizing fasciitis of the perineum and genital region frequently due to a synergistic polymicrobial infection [1–5]. This truly emergent condition is typically seen in elderly, diabetic, or otherwise immune compromised individuals [1–5]. Here, we report an unusual case of Fournier’s gangrene due to excessive masturbation in an otherwise healthy 29-year-old male
HOW COMMON IS IT?

Fournier’s gangrene is rare. While it’s more common in men, women and children also can get it. The disease is most often found in men between the ages of 50 and 60. Men are 10 times more likely than women to have Fournier’s gangrene. Fournier’s gangrene is even rarer in children. Treatment usually consists of the surgical removal (debridement) of extensive areas of dead tissue (necrosis, necrotic) and the administration of broad-spectrum intravenous antibiotics. Surgical reconstruction may follow where necessary.
SIGNS AND SYMPTOMS

Symptoms include fever, general discomfort (malaise), moderate to severe pain and swelling in the genital and anal areas (perineal) followed by rankness and smell of the affected tissues (fetid suppuration) leading to full blown (fulminating) gangrene. Rubbing the affected area yields the distinct sounds (crepitus) of gas in the wound and of tissues moving against one another (palpable crepitus). In severe cases, the death of tissue can extend to parts of the thighs, through the abdominal wall and up to the chest wall. This disease is commonly found in conjunction with other disorders (comorbidity), especially those that weaken the immune system. Some disorders that increase the predisposition to Fournier gangrene are diabetes mellitus, profound obesity, cirrhosis, interference with the blood supply to the pelvis, and various malignancies.
Some disorders that increase the predisposition to Fournier gangrene are diabetes mellitus, profound obesity, cirrhosis, interference with the blood supply to the pelvis, and various malignancies.
CAUSES
Portals of entry for the bacteria, fungi, and/or viruses responsible for a particular case of Fournier gangrene are generally colorectal, urogenital or cutaneous in origin.
Anorectal abscesses, urinary tract infections, surgical instrumentation and other contributing factors have all been implicated. Some cases continue to be of unknown cause (idiopathic).
Why this process occasionally develops in individuals with common ailments is still not understood.
- Case Presentation
An otherwise healthy 29-year-old male presented to the emergency department (ED) after being evaluated at an outside urgent care clinic for two days of fever, vomiting, and diffuse myalgias. Upon further questioning, he also endorsed severe scrotal pain and swelling and frequent masturbation with soap as a lubricant.
He reported that past episodes of masturbation often resulted in recurrent penile erythema and abrasions which had worsened over the previous three days since his last masturbation episode. He denied any recent travel, notable lapses in personal hygiene, or any other preceding genitourinary injury or symptoms.
The patient appeared alert but ill and in pain, with rigors and a rectal temperature of 104.3°F. His initial blood pressure was 87/50?mmHg, heart rate was 124?beats/min, and respiratory rate was 24?breaths/min with an oxygen saturation of 100% on room air.
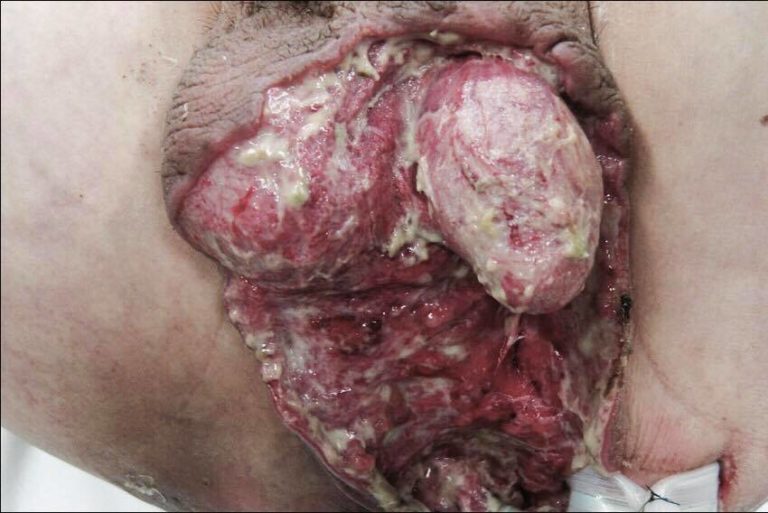
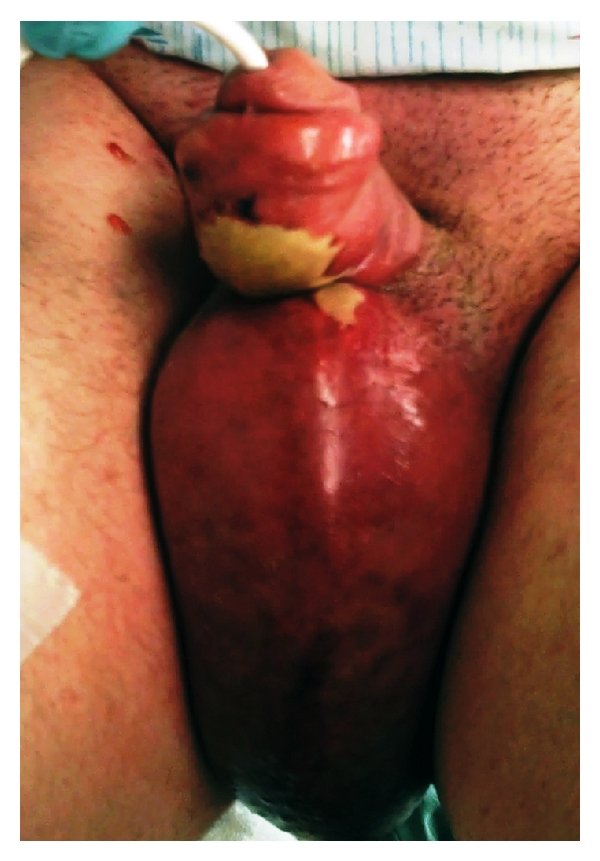
His physical exam was remarkable for significant erythema, edema, and calor of the penis and scrotum extending to the region of the pubis symphysis but sparing the glans (Figure 1). A large malodorous eschar was noted to the ventral surface of the penis.
Aggressive intravenous (IV) fluid resuscitation with normal saline was begun and, with a provisional clinical diagnosis of Fournier’s gangrene, IV clindamycin, and ampicillin/sulbactam, was administered, and surgery was consulted. His initial ED labs were remarkable for a white blood cell count of 12,000/mm3 and a lactate of 2.2?mEq/L.
The patient was taken to the operating room where cystoscopy and anoscopy were found to be normal with no sign of gangrenous extension or source of infection from the bladder or rectum.
He underwent three separate surgical debridements of the scrotum and penis as well as penoscrotal split-thickness skin grafting. Intravenous immunoglobulin (IVIG) was added to his treatment regimen and blood cultures identified strains of Staphylococcus aureus and Streptococcus pyogenes. On hospital day 22, he was discharged home.