Angina Pectoris: Are You Wary of that Silent Killer?
The modern day generation has witnessed dynamism in terms of events and discoveries, revolutionary breakthrough and of course, agonies of natural disasters predominantly among which are hurricanes, earthquakes and tsunami; and plagues which range from common cholera to HIV and to some extent, Ebola. But there exists a previously trivialized health condition which has managed to burrow into the mainstream of global health concerns thereby posing as a silent but giant killer everyone must struggle to defeat or better still, avoid at all costs. Its name is angina pectoris, known or unknown.

What is Angina?
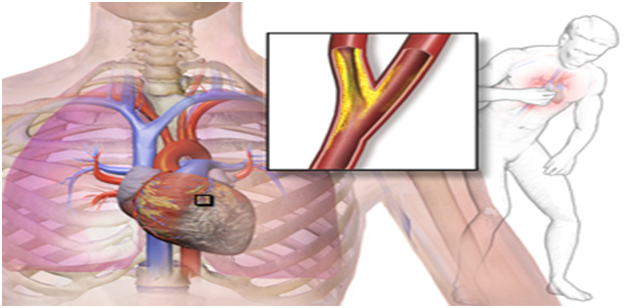
The term angina derives its name from Latin word “angere”, which means “to strangle” and pectoris from “pectus” meaning “chest”. There we can translate it as a strangling feeling in the chest. Angina which is known as angina pectoris is a pain or pressure in the chest as a result of shortage in the flow of blood to muscles of the heart. It mostly results when there is an imbalance between the demand and supply of oxygen for the heart especially during a physical exercise. This, in turn might be caused by an obstruction or narrowing (atherosclerosis) of the coronary arteries of the heart. It is also called ischemic chest pain and it occurs when the heart doesn’t get as much blood and oxygen as it needs because one or more arteries are narrowed or blocked and the pain is triggered by strenuous physical activities or emotional stress.
Angina can be quite severe and this was known as a sign of an impending death in the early 20th century. Though heart attack can occur without chest pain, and there can be severe pain with little or no risk of heart attack, yet majority of myocardial infarction (heart attack) cases have been preceded by worsened angina attacks.
The main agents of coronary artery obstruction are an atherosclerosis or simply put cholesterols and other fats buildups in and on the wall of arteries and cause them to narrow severely. However females do experience non-coronary disease. This requires a medical diagnosis to determine.
Though the outlook has improved significantly given the current medical therapies, people with average of 62 years of age who are having moderate to severe conditions of angina have average of 5 years rate of survival, which approximates 92%. In the US alone in 2010 10.2 million are estimated to experience angina with approximately 500,000 new cases occurring each year, of which 4.8% of individuals with angina later died from coronary heart disease. And they are mostly men. This bears similar figure with the rest of the western world and later China. This is due to the people’s diets and lifestyle.
Symptoms of Angina
Angina has a lot of symptoms which vary according to individual’s severity and condition but most prominent among them are the following classes.
- Typical symptoms
- Atypical symptoms
Typical Symptoms
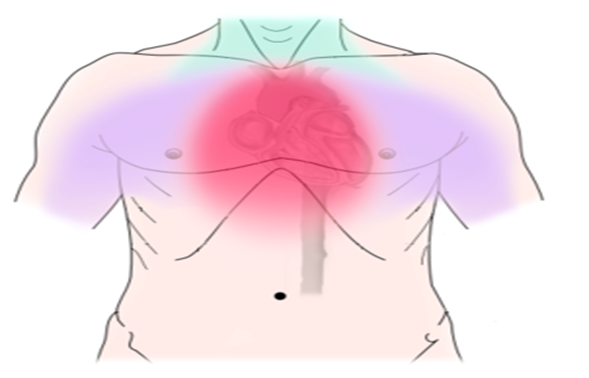
These include chest pain, chest discomfort and not even pain in some patients. These discomforts are often described as heaviness, pressure, tightness, and burning, squeezing and choking sensation. Oftentimes angina pains may extend to the back area, jaw and shoulders, upper central abdomen and neck area.
Atypical symptoms
These are often presented by patients of older age, women, and diabetic patients. They include nausea, burning in the chest and breathlessness.
Types of angina
There are two main types of angina and they are
- Stable angina and
- Unstable or crescendo angina
Stable Angina
This is the most common and elementary type or stage of angina. It is a predictable type which pattern of chest pain can be tracked based on pattern of activities the patient does when he or she feels the chest pain. This makes stable angina easier to manage. Even though it poses less threat to the patient it is still advisable to seek a thorough medical analysis and intervention to prevent its aggravation.
Unstable Angina
This type is a changed or worsened acute coronary syndrome. It often lasts more than 15 minutes. It’s of severely new onset (occurs within the prior 4-6 weeks) and it occurs more severe, prolonged or more frequent than before. It may also occur unpredictably at rest, which could seriously indicate a looming heart attack. Its pathophysiology is a reduced coronary flow which results from transient platelets that aggregate on apparently normal endothelium, coronary thrombosis or spasm of coronary arteries. This may cause cell necrosis (infarction) if it is not reversed. The fibrous cap which protects the developing atheroma may rupture in unstable angina and allows blood clots to precipitate and decrease further, the lumen area of the coronary vessels. All these require urgent medical intervention as they may precede a heart attack.
Angina’s Risk Factors
There are many factors that expose people to angina but prominent among them are the following.
- Prolonged psychological stress
- Kidney disease
- History of cardiovascular disease in the family
- Hypertension
- Age (45+ years in men and 55+ years in women)
- Obesity
- Smoking and lifestyle
- Physical inability
- Diabetes mellitus
- Uncontrolled strenuous physical exercise
- Diets - This is evident in the common cases of angina in the west and westernized countries. This happens due to their adoption of rich diets which easily trigger obesity as against the third world where coronary heart diseases are not much common due to poverty and inability to afford rich diets.
Treatments for Angina
Angina treatment could not be achieved without first looking back at its causes and more importantly, the type of angina that occurs. Generally speaking your chest pain is caused by blockages in your heart’s arteries and you’ve got to take care of those blockages to allow an improved flow of blood and require oxygen to the heart. So we weigh the options we have. It is important to note that the most common types are chronic class of stable angina which occurs when the heart works hard, new cases of unstable which occur with new chest pains and ones that are degenerating. Another uncommon but noteworthy class are the ones caused by spasms in the coronary arteries and also a microvascular angina which can be a symptom of disease of small coronary artery blood vessels
The most common angina medicine is nitroglycerin because of its potency in decreasing myocardial oxygen demand by reducing heart’s workload. However nitroglycerin inhibitors such as sildenafil, tadalafil or vedenafil must not have been taken within the previous twelve hours. This is because their combination could cause a serious reduction in blood pressure.
A gentle and sustained exercise is also a long-term treatment for angina. This is important in improving blood pressure and promoting coronary arteries collateralization.
A low-dose of aspirin equally decreases the risk of heart attack in patients suffering from chronic stable angina and it has been used as standard treatment.
Another method of treatment is balloon angioplasty. Here the balloon will be inserted at the end of catheter and inflated to widen the arterial lumen. This is used at the same time with stents to maintain arterial widening.
Unstable angina is a serious situation and requires an emergency treatment that involves hospitalization with medication in order to stabilize the condition. In some extreme cases a heart surgery for coronary bypass may be needed. This involves bypassing narrowed arteries with venous graft. This is more invasive than angioplasty and makes the last resort since the goal is to prevent heart attack and eventual death.
Note: no evidence has supported the use of traditional Chinese herbal products for treatment of angina. Though they are sometimes used by patients.
Summary
The best recommendation is identifying and treating the risk factors through testing for elevated cholesterols and other fats in the blood, hypertension and diabetes, optimization of weight and cessation of smoking. Early stages of chest discomfort should be reported at competent medical facilities.
Legal Disclaimer
This write up represents an extract from the research conducted by the author and should not necessarily be used as a measure of outright diagnosis and treatment. Always consult your doctor for medical advice.