Technique for incision and drainage of subcutaneous abscess
Warning some images may be a bit disturbing
Next I am going to share a simple and straightforward technique that is carried out by both in-hospital and out-patient staff, at the hands of trained doctors, I hope you will find it enjoyable and useful.
Subcutaneous abscesses are one of the most common injuries affecting the general population, and these in turn can be distributed over a wide area of the body and this will depend on the etiological agent and immune capacity of the individual.
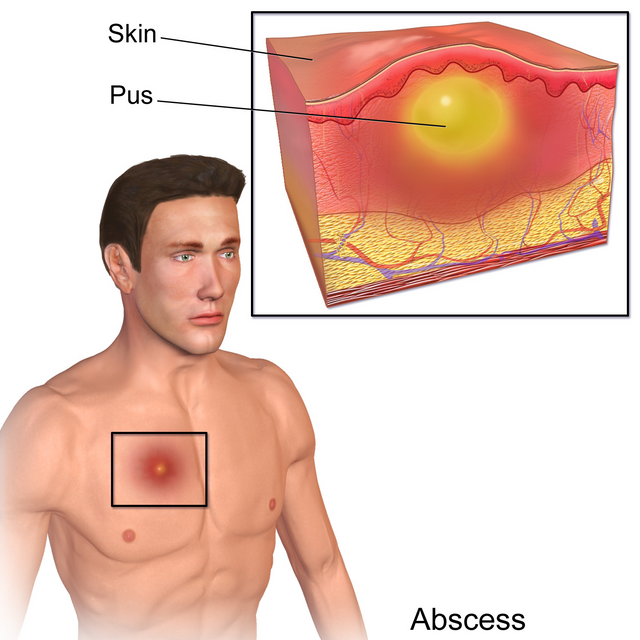
Generally speaking, an abscess is a painful, fluctuating mass that covers the epidermis and dermis layers of the skin, accompanied by the typical signs given by flushing, heat and pain, also called signs of phlogosis.

U.S. Army photo By Marcy Sanchez. Public domain
Incision and drainage of an abscess is the definitive treatment of a soft tissue abscess, prior to the administration of antibiotic therapy, which aims to significantly improve symptoms and rapidly resolve the local infection.
However, to carry out this technique it is necessary that the abscess is fluctuating, that is why it is essential to administer oral or endovenous antibiotic therapy, so that the lesion takes these characteristics and is suitable for drainage.
Anatomy
The skin is the largest and most extensive organ, which completely covers the human body, exerts vital protective functions, maintains the balance of body fluids, thermal, rich in sensory innervation and that, through them, we can express our emotional state as, for example, when we blush, skin pallor, pheromone secretion.
Composition
Epidermis layer that is exposed to the environment, made up of a flat, polystyrene and keratinized epithelium, which gives the skin resistance, with respect to temperature, external pH and certain substances.
Dermis is the second layer of the body, whose function is support, resistance and elasticity, this is because it is made up of fibroelastic connective tissue. In addition, it is richly vascularized, so that through it the epidermis is nourished.
The skin's annexes are made up of a wide variety of structures, including hair, sebaceous glands, sweat glands and finally the nails.
Subcutaneous tissue or hypodermis with variable thickness and which does not have a defined limit in relation to the dermis, through which numerous terminations flow and we go sanguine in addition it is a source of energy storage, thermal insulator and mechanical protector.
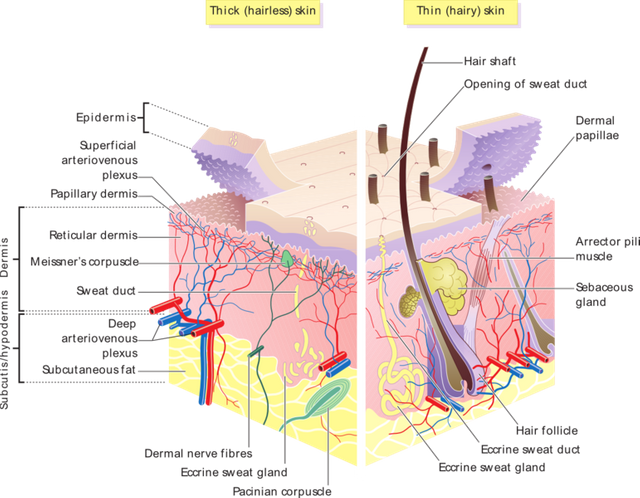
Skin layers. Licensed wikipewdia CC BY-SA 3.0
Pathogenesis
An abscess is an accumulation of pus located in a tissue, organ or confined space due to a discharge from an infectious site. Localized pyogenic infections usually begin after the skin's defense mechanisms have broken down.
The occlusion of the ducts of the superficial exocrine glands, such as the sebaceous, apocrine and even cyst glands or congenital sinuses, can initiate this infectious process. This occlusion prevents desquamation and provides a humid environment suitable for local bacterial proliferation.
The combination of a high concentration of microorganisms, the presence of nutrients and sufficient damage to the layers of the skin, especially the corneal layer which is part of the epidermis, allows the entry of microorganisms and growth.
Abscesses can start as a cellulite with microorganisms capable of generating necrosis, lichenification and accumulation of leukocytes and cell debris. The initial stages of the local infection are characterized by an area of hyperemia and painful inflammation that with the days becomes fluctuating and this happens as leukocyte exudates, necrotic material and cellular remains accumulate. As the process progresses, the area of lichenification increases until it protrudes and goes to the outside, which is the area of least resistance.
The areas of the body involved depend on host factors, such as intravenous drug use, exposure to certain agents, or the presence of local trauma.
The areas most often involved are first:

Skin infection. Public domain image
Etiological agent
Most abscesses are polymicrobial, and that depends on the anatomical area where the abscess is located, where the pathogen is mostly normal bacterial flora but for special situations invades and colonizes.
Abscesses with non-resident bacteria are usually the result of direct inoculation of these bacteria from the outside, as occurs in cases of bites, use of intravenous drugs or planting of bacteria after the embedding of foreign bodies.
The most frequent pathogens isolated are Staphylococcus, Group A Streptococcus are usually the agents involved in head, neck, limb and trunk abscesses, while aerobic bacteria are involved in abscesses of the buttocks and peri rectal area.
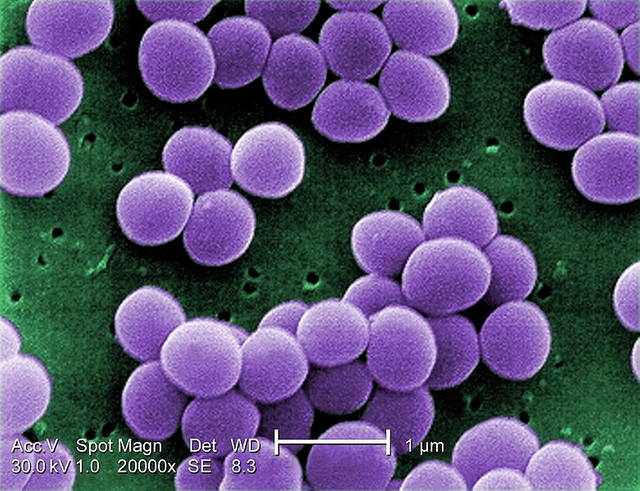
In relation to Staphylococcus aureus, it is responsible for infectious processes in soft tissues with an estimated more than 60%. Immunocompromised patients, such as HIV carriers, diabetes mellitus, leukemia, and transplant recipients among others, present a greater risk of abscess formation, which in turn are usually serious clinical presentations.
These hosts are also predisposed to suffer infections by atypical microorganisms (fungi, parasites, sepa blee bacteria) with little sensitivity and response to antibiotic therapy. In those cases, empirical treatment should be considered with subsequent taking of cultures of the secretion obtained and the referral of surgical cleaning and continuous follow-up of these patients should be considered.
Specific clinical entities
Boils or bullae are acute abscesses confined to the skin and subcutaneous tissue, most frequently located on the face, neck, buttocks, thigh, perineum, chest and armpit.
Carbunculosis represents a conglomerate of interconnected boils, located under the thick skin of the back, are large in size and extension in some cases can trigger systemic processes, usually affecting diabetic patients.

Hidroadenitis suppurativa is a chronic and recurrent inflammation of the apocrine glands, mainly those located in the armpit and inguinal region, it can lead to the formation of fistulas that require surgical treatment. These are recurrent lesions that, despite receiving antibiotic therapy and drainage, are frequent to appear with time.
With regard to breast abscesses, more than 80% affect patients who are not breastfeeding and even to a lesser extent in men, cases have been reported, are similar to injuries on any other side of the body, with good response empirical treatment and drainage of the injury. In relation to postpartum mastitis where the bacterial invasion occurs through the cracked nipple allowing the passage and proliferation of microorganism, in these cases it is essential the use of oral or intravenous antibiotics according to the severity of the case, plus continuous emptying of the breast with suction pump.
Finally, sebaceous cysts are a frequent cause of subcutaneous abscesses, can even remain as painless masses, for a long time until they are infected, are easy to identify because it observes a small duct located near the fluctuating area, the treatment of choice is the incision and drainage of the same, these have bright white capsule covering the abscess which must be removed at the time of executing its extraction.
It should be noted that the presence of recurrent abscesses suggests the possibility of underlying osteomyelitis, foreign body retention or the presence of an unusual etiological agent.
Indications
The presence of a fluctuating mass in the indurated area, with clinical evidence of abscesses, requires an incision and drainage. If there is any doubt that it is not an abscess with an infectious etiology, it is essential to puncture it and aspirate its contents to confirm the presence of an abscess. If pus is obtained during aspiration, an immediate incision and drainage is recommended.
If pus is not obtained, it is recommended to administer antibiotics, use local warm compresses and reassess after 24 hours.
Public domain licensed CC BY-SA 3.0
Contra-indications
The only absolute contraindication to perform this technique is the presence of a fungal aneurysm, or that are located above a large vessel, as in the case of its location in neck, supraclavicular fossa, groin and popliteal space, in these cases an angiography prior to the incision is useful and ideally fine needle aspiration.
Abscesses associated with deep-seated foreign bodies require prior studies such as ultrasound and, in some cases, referral for minor surgery.
It is contraindicated in situations such as, infectious processes involving neurovascular or tendon structures, deep infections such as necrotizing fasciitis, myonecrosis, facial abscesses, periorbital is not recommended for use.
Preparing the patient
Always before performing any technique it is important to explain to the patient the procedure, its risks and benefits. We must obtain informed consent before starting the procedure.
It starts with the asepsis and antisepsis of the area to perform the technique, povidone-iodine is applied to the skin and let it dry, or as an alternative any other antiseptic solution. Delimit a sterile field with surgical sheets.
Anesthesia

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Its use is controversial, since the infiltration of local anesthesia in the infected tissues is usually low and delays its action in the tissue, therefore, its indication is not very effective.
Another technique with greater effectiveness is to perform a regional blockade by subcutaneously injecting a ring of 1% lidocaine or 0.5% bupivacaine 1 cm from the perimeter of the lesion.
There are other methods, such as spray anesthesia on the lesion, which is useful in cases of superficial involvement.
The application of local elastic ice bags for 15 minutes can also be effective.
Fentanyl and midazolam may be appropriate sedatives during deep abscesses that require extensive exploration.
Technique
Aspiration
Useful for determining the presence of a fluctuating abscess whose interior is filled with pus, and even for taking culture samples from the lesion. By itself this is not a therapeutic intervention.
Introduce the needle number 18 of a 10 ml syringe, on the fluctuating base of the lesion, in case pus is obtained, the collection of cultures and the incision and drainage of the abscess must proceed.
If blood is aspirated, the technique should be stopped, pressure should be applied to the area to avoid the formation of hematoma and a referral should be made to a physician specialized in these cases for extension studies.
If no blood or pus is aspirated, redirect the needle in various directions until the absence of the abscess is confirmed. Indicate oral antibiotics and reassess after 48 hours.
Incision and drainage
An incision is made either parallel to the skin tension lines, completely covering the fluctuating area, this being the most aesthetic technique, or an elliptical incision can also be made, which allows a thick layer of tissue to be removed and the wound to be kept open, this is not recommended in cosmetic areas such as the face, neck and chest.

Skin abscess incision and drainage. Public domain
Debridement of the necrotic or devitalized tissue, explore the cavity, inserting haemostatic tweezers, in order to break any partition or pus-filled sac, remove the bright white capsule in case of sebaceous cyst.
Finally, irrigate the abscess cavity with physiological solution or saline, fill the abscess cavity with gauze impregnated with iodine in case it is not contraindicated (allergic reactions) and proceed to cover the wound.
Finally, complications secondary to the technique are rare, usually unwanted scars and aesthetic involvement, and if they are not carried prior asepsis and antisepsis and staff entered the overinfection is often accompanied by systemic infection, these cases are more common in immunocompromised patients, either by HIV, diabetes mellitus, neoplasms, Les, among others.
Sources:

steemSTEM is a project of the chain of blocks that supports the scientific content in different areas of science. If you want to know more about this wonderful project you can join the server in discord
This article will be published at https://www.steemstem.io/
link
If you have any questions about any topic of medicine or present any disease you can comment the publication or write me in discord and I will attend you.
Dr. Ana Estrada
I hope you enjoyed my content.
@tipu curate
Upvoted 👌 (Mana: 0/10 - need recharge?)
Thank you very much :)
This post has been voted on by the SteemSTEM curation team and voting trail. It is elligible for support from @curie and @minnowbooster.
If you appreciate the work we are doing, then consider supporting our witness @stem.witness. Additional witness support to the curie witness would be appreciated as well.
For additional information please join us on the SteemSTEM discord and to get to know the rest of the community!
Please consider using the steemstem.io app and/or including @steemstem in the list of beneficiaries of this post. This could yield a stronger support from SteemSTEM.
Thank you very much @steemstem for support
Congratulations @anaestrada12!
You raised your level and are now a Minnow!
Do not miss the last post from @steemitboard:
Your level lowered and you are now a Red Fish!
Do not miss the last post from @steemitboard:
Hi, thanks for the post! I included a link to it in my daily Science and technology digest, and you'll get a 10% share of that post's rewards.
Great congratulations, doctor.... @remlaps-lite summaries are excellent
I appreciate it very much :)
Excellent technique very well described
Thank you Carlos